

The therapeutic age of the neonatal Fc receptor
- PMID: 36726033
- PMCID: PMC9891766
- DOI: 10.1038/s41577-022-00821-1
The therapeutic age of the neonatal Fc receptor
Abstract
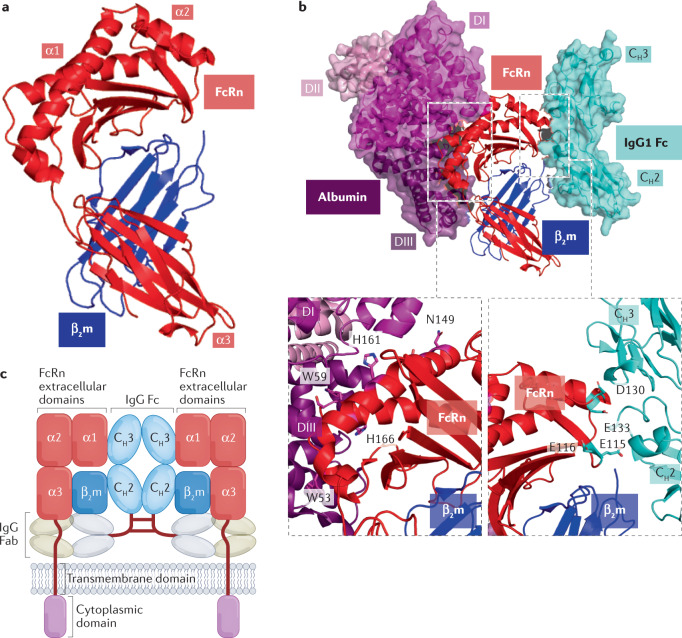
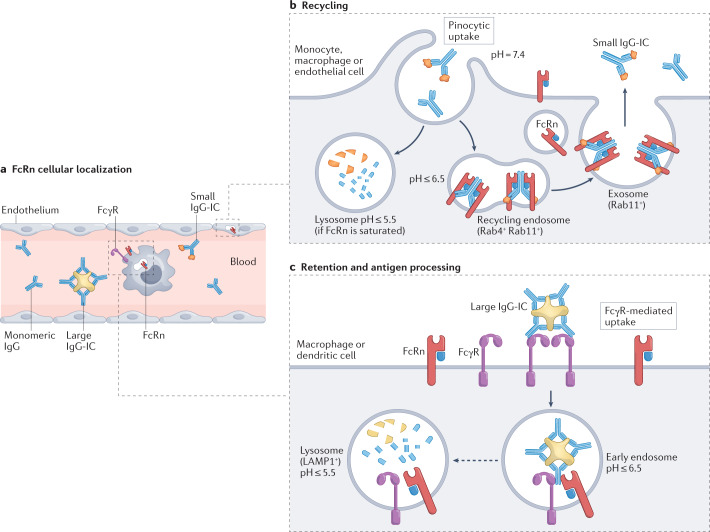
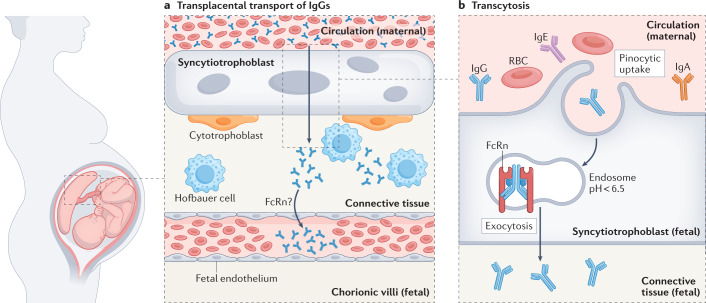
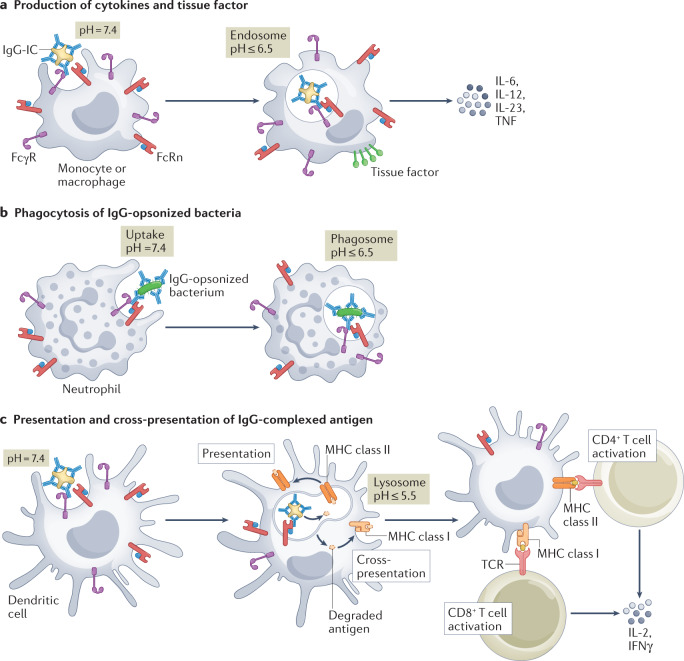
IgGs are essential soluble components of the adaptive immune response that evolved to protect the body from infection. Compared with other immunoglobulins, the role of IgGs is distinguished and enhanced by their high circulating levels, long half-life and ability to transfer from mother to offspring, properties that are conferred by interactions with neonatal Fc receptor (FcRn). FcRn binds to the Fc portion of IgGs in a pH-dependent manner and protects them from intracellular degradation. It also allows their transport across polarized cells that separate tissue compartments, such as the endothelium and epithelium. Further, it is becoming apparent that FcRn functions to potentiate cellular immune responses when IgGs, bound to their antigens, form IgG immune complexes. Besides the protective role of IgG, IgG autoantibodies are associated with numerous pathological conditions. As such, FcRn blockade is a novel and effective strategy to reduce circulating levels of pathogenic IgG autoantibodies and curtail IgG-mediated diseases, with several FcRn-blocking strategies on the path to therapeutic use. Here, we describe the current state of knowledge of FcRn-IgG immunobiology, with an emphasis on the functional and pathological aspects, and an overview of FcRn-targeted therapy development.
© 2023. Springer Nature Limited.
Conflict of interest statement
R.S.B. had equity interests in Syntimmune Inc., a company developing therapeutic agents to target FcRn. Syntimmune Inc. was a wholly owned subsidiary of Alexion Pharmaceuticals Inc., which was acquired by AstraZeneca. M.P., L.K.K. and A.G. declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
