

Clinicopathological characteristics and disease chronicity in native kidney biopsies in Flanders
- PMID: 36726429
- PMCID: PMC9871845
- DOI: 10.1093/ckj/sfac208
Clinicopathological characteristics and disease chronicity in native kidney biopsies in Flanders
Abstract
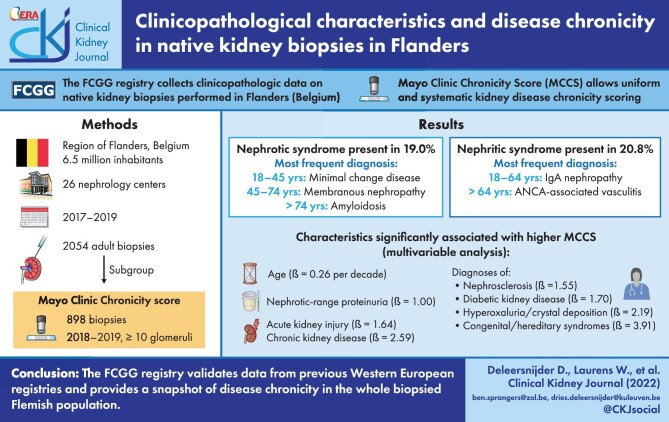
Background: The Flemish Collaborative Glomerulonephritis Group (FCGG) registry provides complete population data on kidney disease epidemiology in the region of Flanders (Belgium), as it captures all native kidney biopsies performed in its population of 6.5 million inhabitants.
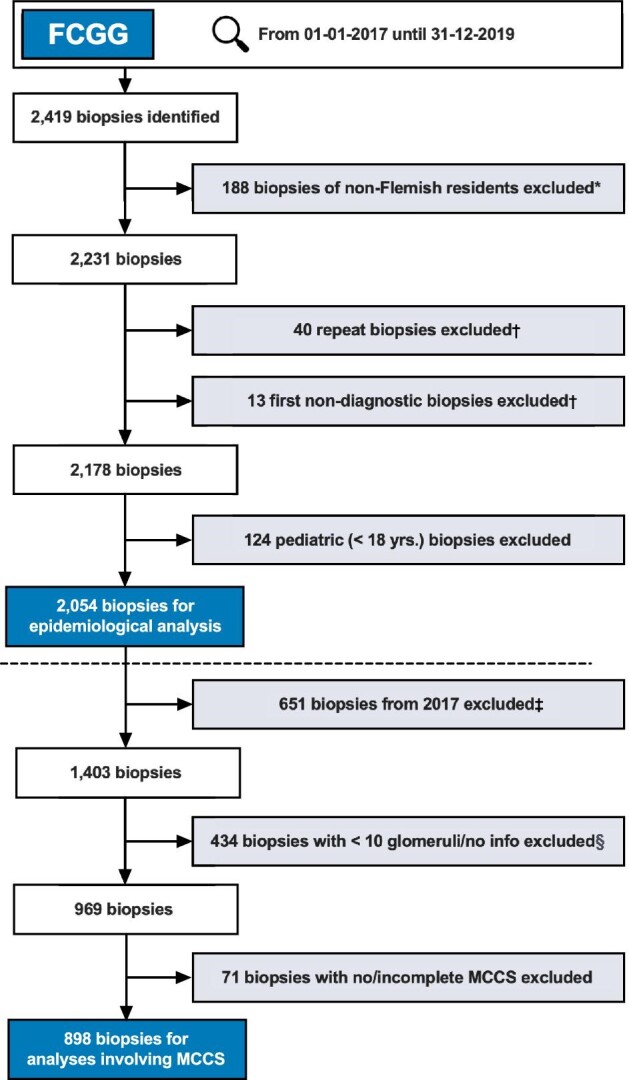
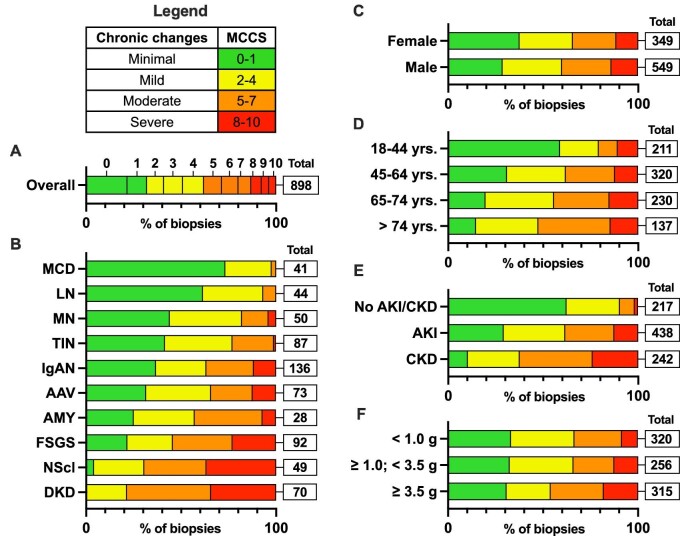
Methods: From 2017 until 2019, 2054 adult kidney biopsies were included from 26 nephrology centers (one biopsy per patient). Data on nephrotic and nephritic syndrome were available in 1992 and 2026 biopsies, respectively. In a subgroup of 898 biopsies containing ≥10 glomeruli from 2018 to 2019, disease chronicity was graded using the Mayo Clinic Chronicity Score (MCCS). The association between clinical variables and MCCS was determined using simple and multiple linear regression models.
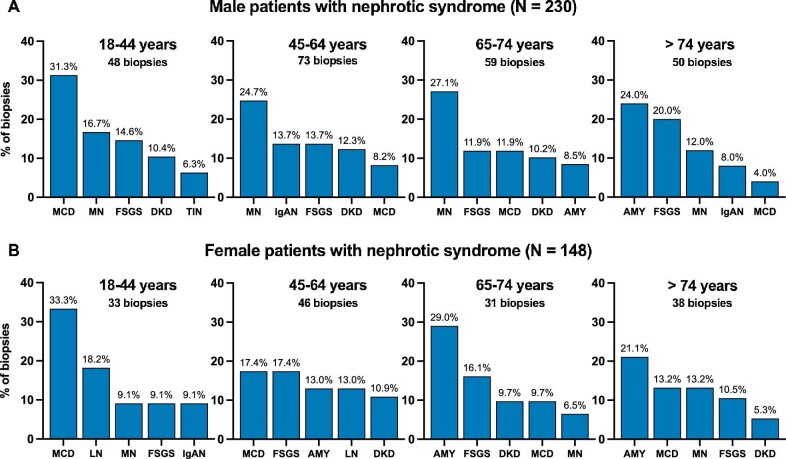
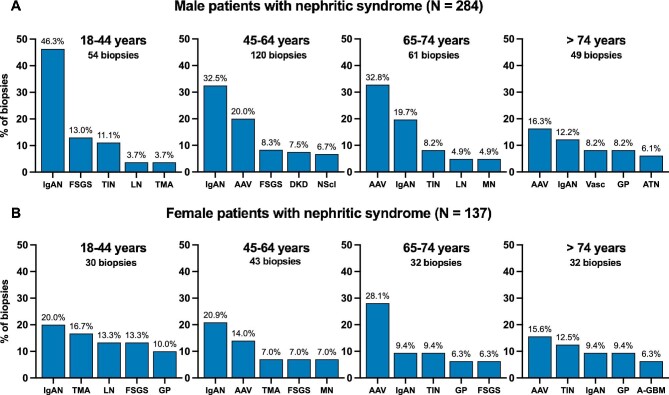
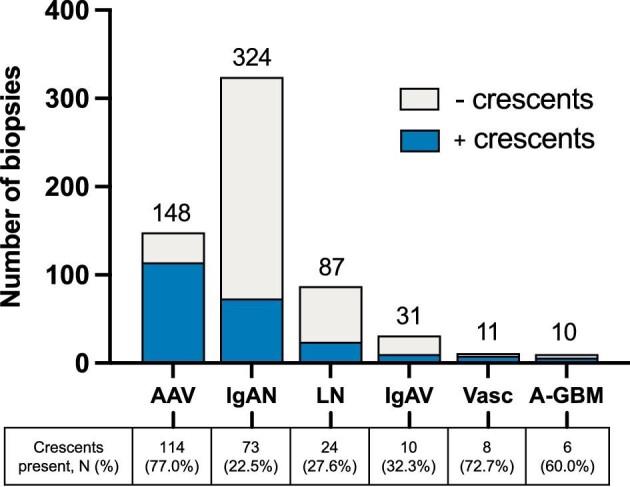
Results: Nephrotic syndrome (present in 378 patients, 19.0%) was most frequently caused by minimal change disease in younger patients (18-44 years), membranous nephropathy in older patients (45-74 years) and amyloidosis in the elderly (>75 years). Nephritic syndrome (present in 421 patients, 20.8%) was most frequently caused by immunoglobulin A nephropathy (IgAN) in younger patients (18-64 years) and ANCA-associated vasculitis (AAV) in older patients (>64 years). AAV and IgAN were the most frequent underlying diagnoses in biopsies in which crescents were identified. In multivariable analysis, acute and chronic kidney disease and diagnoses of diabetic kidney disease, nephrosclerosis and hyperoxaluria/hypercalcemic nephropathy were associated with the highest MCCS increases.
Conclusions: The FCGG registry validates data from previous Western European registries and provides a snapshot of disease chronicity in the whole biopsied Flemish population.
Keywords: MCCS; chronicity; epidemiology; kidney biopsy; registry.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
LinkOut - more resources
Full Text Sources
