

Host immunological responses facilitate development of SARS-CoV-2 mutations in patients receiving monoclonal antibody treatments
- PMID: 36727404
- PMCID: PMC10014108
- DOI: 10.1172/JCI166032
Host immunological responses facilitate development of SARS-CoV-2 mutations in patients receiving monoclonal antibody treatments
Abstract
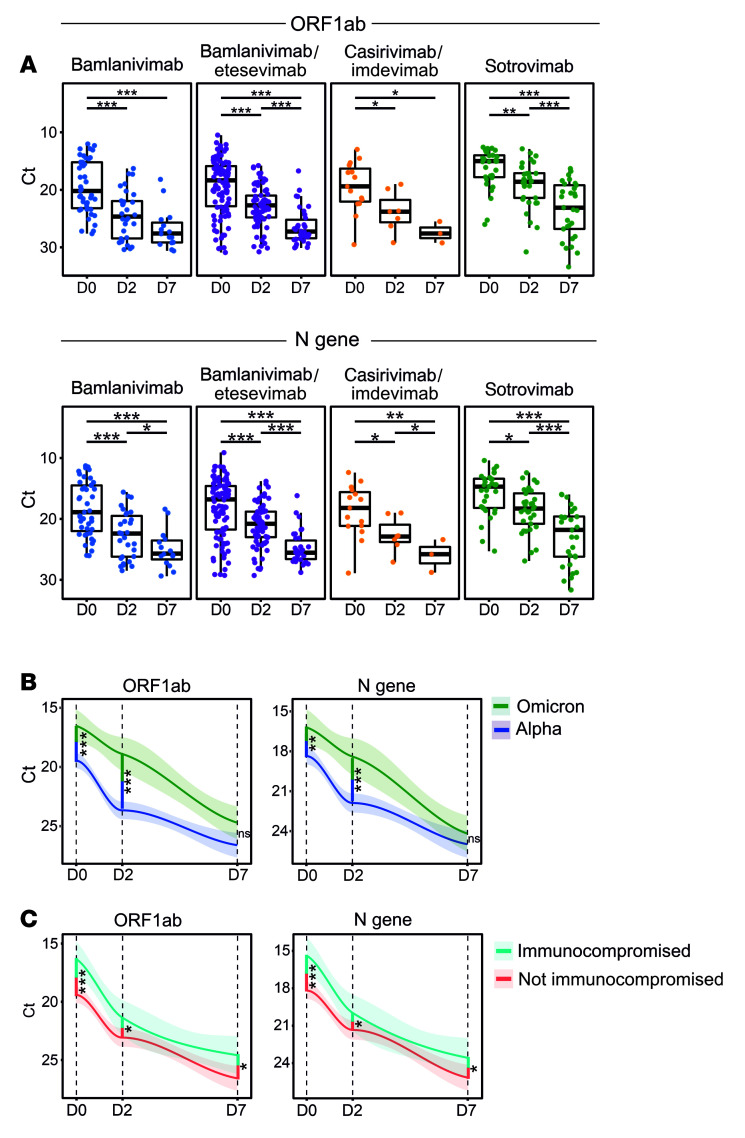
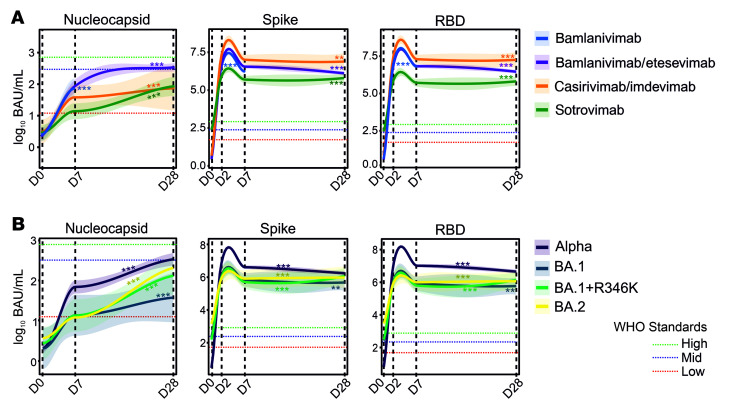
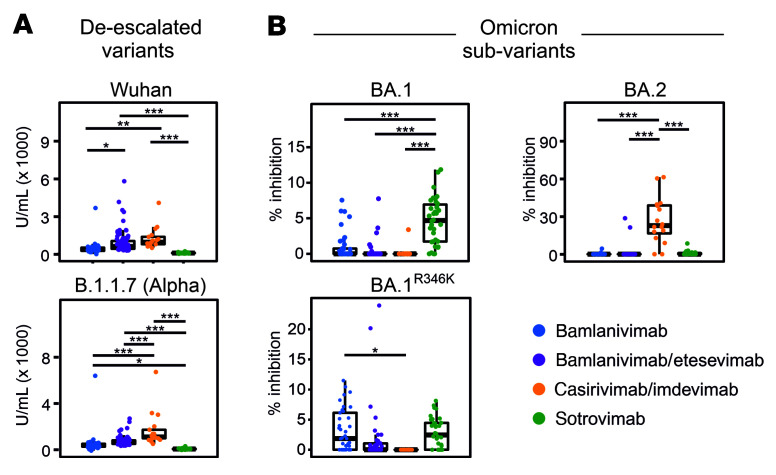
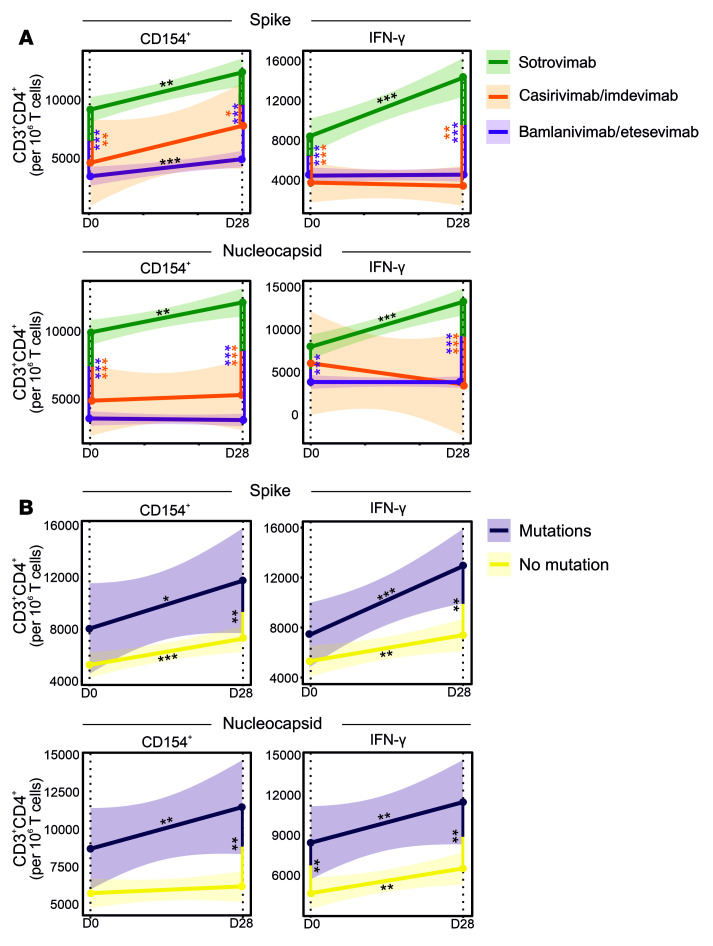
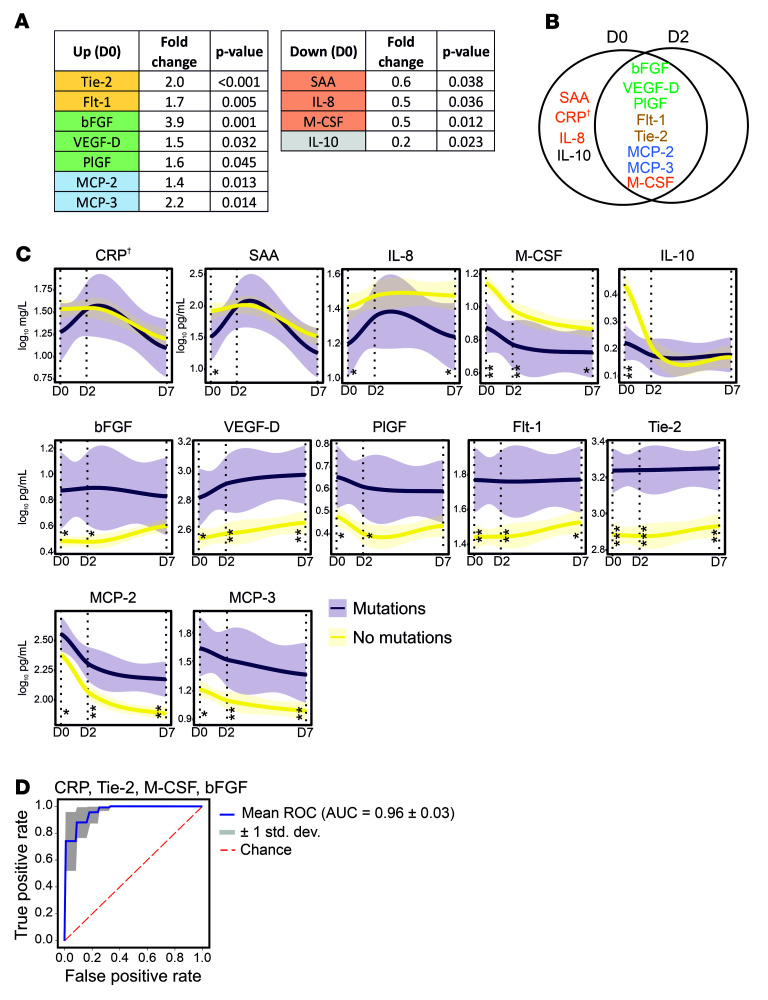
BackgroundThe role of host immunity in emergence of evasive SARS-CoV-2 Spike mutations under therapeutic monoclonal antibody (mAb) pressure remains to be explored.MethodsIn a prospective, observational, monocentric ORCHESTRA cohort study, conducted between March 2021 and November 2022, mild-to-moderately ill COVID-19 patients (n = 204) receiving bamlanivimab, bamlanivimab/etesevimab, casirivimab/imdevimab, or sotrovimab were longitudinally studied over 28 days for viral loads, de novo Spike mutations, mAb kinetics, seroneutralization against infecting variants of concern, and T cell immunity. Additionally, a machine learning-based circulating immune-related biomarker (CIB) profile predictive of evasive Spike mutations was constructed and confirmed in an independent data set (n = 19) that included patients receiving sotrovimab or tixagevimab/cilgavimab.ResultsPatients treated with various mAbs developed evasive Spike mutations with remarkable speed and high specificity to the targeted mAb-binding sites. Immunocompromised patients receiving mAb therapy not only continued to display significantly higher viral loads, but also showed higher likelihood of developing de novo Spike mutations. Development of escape mutants also strongly correlated with neutralizing capacity of the therapeutic mAbs and T cell immunity, suggesting immune pressure as an important driver of escape mutations. Lastly, we showed that an antiinflammatory and healing-promoting host milieu facilitates Spike mutations, where 4 CIBs identified patients at high risk of developing escape mutations against therapeutic mAbs with high accuracy.ConclusionsOur data demonstrate that host-driven immune and nonimmune responses are essential for development of mutant SARS-CoV-2. These data also support point-of-care decision making in reducing the risk of mAb treatment failure and improving mitigation strategies for possible dissemination of escape SARS-CoV-2 mutants.FundingThe ORCHESTRA project/European Union's Horizon 2020 research and innovation program.
Keywords: COVID-19; Cellular immune response.
Figures

Comment in
- SARS-CoV-2 variants resistant to monoclonal antibodies in immunocompromised patients constitute a public health concern
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
