

Rapid Activation of Neuroinflammation in Stroke: Plasma and Extracellular Vesicles Obtained on a Mobile Stroke Unit
- PMID: 36727508
- PMCID: PMC10052772
- DOI: 10.1161/STROKEAHA.122.041422
Rapid Activation of Neuroinflammation in Stroke: Plasma and Extracellular Vesicles Obtained on a Mobile Stroke Unit
Abstract
Background: Neuroinflammation is ubiquitous in acute stroke and worsens outcome. However, the precise timing of the inflammatory response is unknown, hindering the design of acute anti-inflammatory therapeutic interventions. We sought to identify the onset of the neuroinflammatory cascade using a mobile stroke unit.
Methods: The study is a proof-of-concept, cohort investigation of ultra-early blood- and extracellular vesicle-derived markers of neuroinflammation and outcome in acute stroke. Blood was obtained, prehospital, on an mobile stroke unit. Outcomes were biomarker concentrations, modified Rankin Scale score, and National Institutes of Health Stroke Scale score.
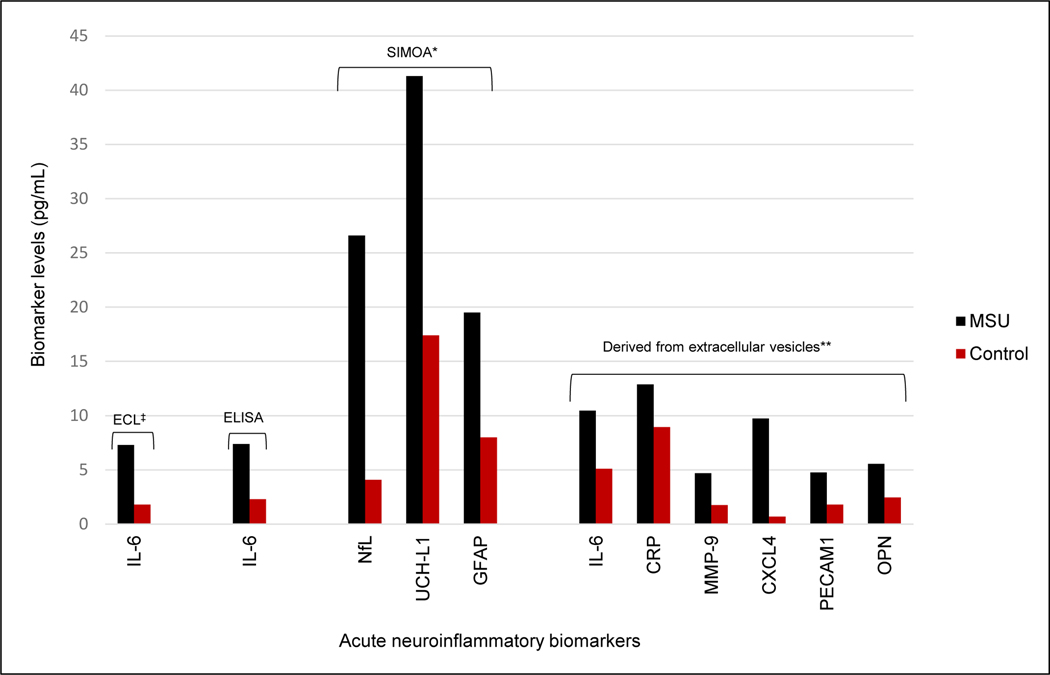
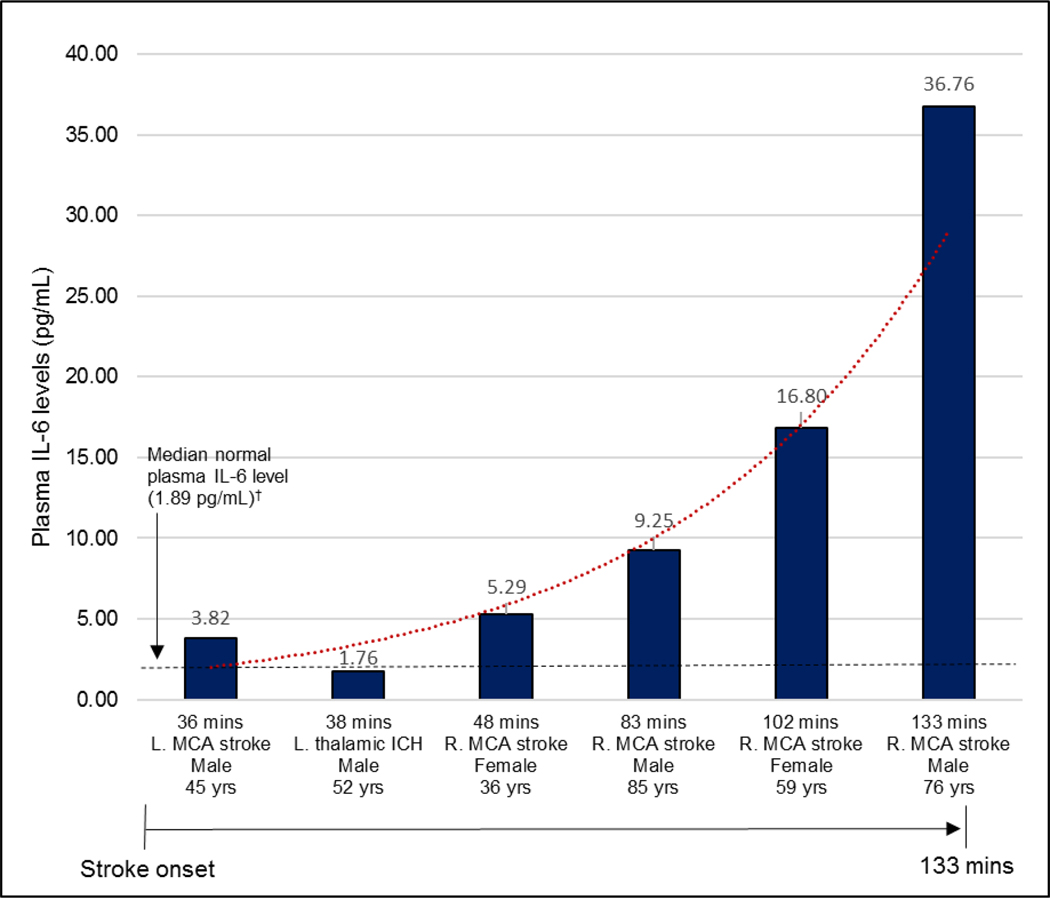
Results: Forty-one adults were analyzed, including 15 patients treated on the mobile stroke unit between August 2021 and April 2022, and 26 healthy controls to establish biomarker reference levels. Median patient age was 74 (range, 36-97) years, 60% were female, and 80% White. Ten (67%) were diagnosed as stroke, with 8 (53%) confirmed and 2 likely transient ischemic attack or stroke averted by thrombolysis; 5 were stroke mimics. For strokes, median initial National Institutes of Health Stroke Scale score was 11 (range, 4-19) and 6 (75%) received tPA (tissue-type plasminogen activator). Blood was obtained a median of 58 (range, 36-133) minutes after symptom onset. Within 36 minutes after stroke, plasma IL-6 (interleukin-6), neurofilament light chain, UCH-L1 (ubiquitin C-terminal hydrolase L1), and GFAP (glial fibrillary acidic protein) were elevated by as much as 10 times normal. In EVs, MMP-9 (matrix metalloproteinase-9), CXCL4 (chemokine (C-X-C motif) ligand 4), CRP (C-reactive protein), IL-6, OPN (osteopontin), and PECAM1 (platelet and endothelial cell adhesion molecule 1) were elevated. Inflammatory markers increased rapidly in the first 2 hours and continued rising for 24 hours.
Conclusions: The neuroinflammatory cascade was found to be activated within 36 to 133 minutes after stroke and progresses rapidly. This is earlier than observed previously in humans and suggests injury from neuroinflammation occurs faster than had been surmised. These findings could inform development of acute immunomodulatory stroke therapies and lead to new diagnostic tools and improved outcomes.
Keywords: adult; biomarker; female; interventions; neuroinflammatory diseases.
Figures
References
-
- Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, Abbasifard M, Abbasi-Kangevari M, Abd-Allah F, Abedi V, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the global burden of disease study 2019. The Lancet Neurology. 2021;20:795–820 - PMC - PubMed
-
- Bustamante A, Penalba A, Orset C, Azurmendi L, Llombart V, Simats A, Pecharroman E, Ventura O, Ribó M, Vivien D, et al. Blood biomarkers to differentiate ischemic and hemorrhagic strokes. Neurology. 2021;96:e1928–e1939 - PubMed
-
- Luger S, Jæger HS, Dixon J, Bohmann FO, Schaefer J, Richieri SP, Larsen K, Hov MR, Bache KG, Foerch C. Diagnostic accuracy of glial fibrillary acidic protein and ubiquitin carboxy-terminal hydrolase-l1 serum concentrations for differentiating acute intracerebral hemorrhage from ischemic stroke. Neurocrit Care. 2020;33:39–48 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
