

A library of quantitative markers of seizure severity
- PMID: 36727552
- PMCID: PMC10952709
- DOI: 10.1111/epi.17525
A library of quantitative markers of seizure severity
Abstract
Objective: Understanding fluctuations in seizure severity within individuals is important for determining treatment outcomes and responses to therapy, as well as assessing novel treatments for epilepsy. Current methods for grading seizure severity rely on qualitative interpretations from patients and clinicians. Quantitative measures of seizure severity would complement existing approaches to electroencephalographic (EEG) monitoring, outcome monitoring, and seizure prediction. Therefore, we developed a library of quantitative EEG markers that assess the spread and intensity of abnormal electrical activity during and after seizures.
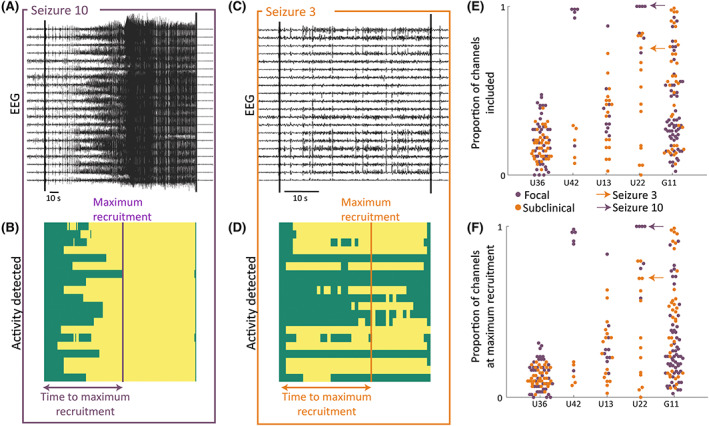
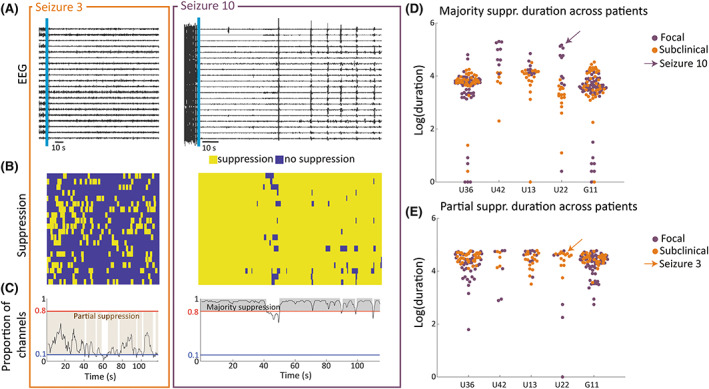
Methods: We analyzed intracranial EEG (iEEG) recordings of 1009 seizures from 63 patients. For each seizure, we computed 16 markers of seizure severity that capture the signal magnitude, spread, duration, and postictal suppression of seizures.
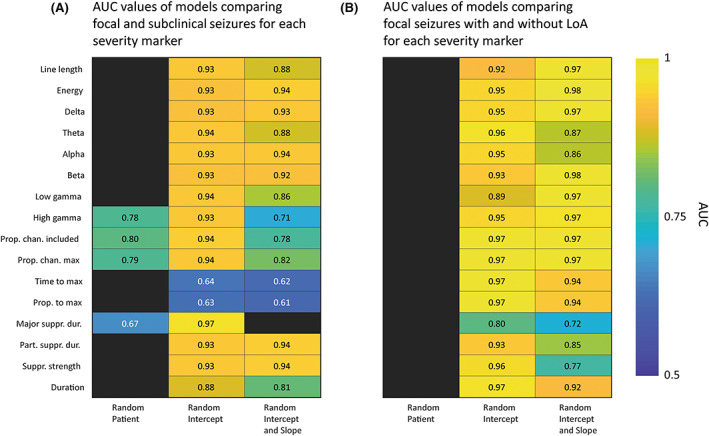
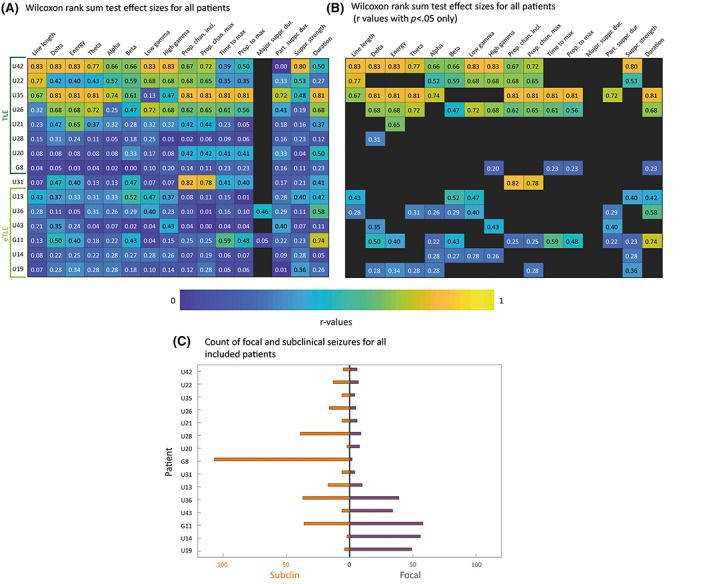
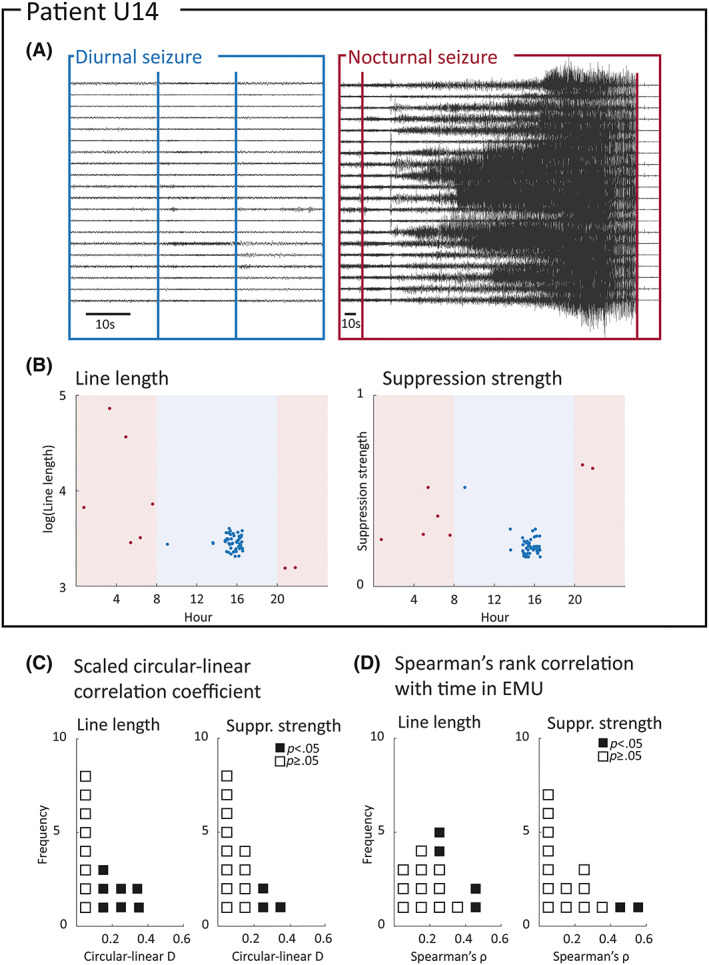
Results: Quantitative EEG markers of seizure severity distinguished focal versus subclinical seizures across patients. In individual patients, 53% had a moderate to large difference (rank sum , ) between focal and subclinical seizures in three or more markers. Circadian and longer term changes in severity were found for the majority of patients.
Significance: We demonstrate the feasibility of using quantitative iEEG markers to measure seizure severity. Our quantitative markers distinguish between seizure types and are therefore sensitive to established qualitative differences in seizure severity. Our results also suggest that seizure severity is modulated over different timescales. We envisage that our proposed seizure severity library will be expanded and updated in collaboration with the epilepsy research community to include more measures and modalities.
Keywords: computational neurophysiology; electroencephalography (EEG); seizure severity.
© 2023 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflict of interest to disclose.
Figures

References
-
- Bautista RED, Glen ET. Seizure severity is associated with quality of life independent of seizure frequency. Epilepsy Behav. 2009;16(2):325–9. - PubMed
-
- O'Donoghue M, Duncan J, Sander J. The national hospital seizure severity scale: a further development of the chalfont seizure severity scale. Epilepsia. 1996;37(6):563–71. - PubMed
-
- Baker GA, Smith DF, Dewey M, Morrow J, Crawford PM, Chadwick DW. The development of a seizure severity scale as an outcome measure in epilepsy. Epilepsy Res. 1991;8(3):245–51. - PubMed
-
- Cramer JA, Baker GA, Jacoby A. Development of a new seizure severity questionnaire: initial reliability and validity testing. Epilepsy Res. 2002;48(3):187–97. - PubMed
