

Anatomical morphology of the aortic valve in Chinese aortic stenosis patients and clinical results after downsize strategy of transcatheter aortic valve replacement
- PMID: 36728213
- PMCID: PMC10106152
- DOI: 10.1097/CM9.0000000000002517
Anatomical morphology of the aortic valve in Chinese aortic stenosis patients and clinical results after downsize strategy of transcatheter aortic valve replacement
Abstract
Background: The study aimed to describe the aortic valve morphology in Chinese patients underwent transcatheter aortic valve replacement (TAVR) for symptomatic severe aortic stenosis (AS), and the impact of sizing strategies and related procedural outcomes.
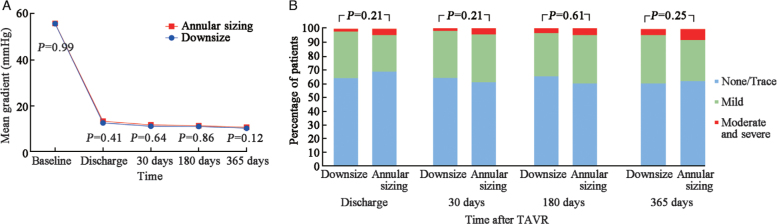
Methods: Patients with severe AS who underwent TAVR were consecutively enrolled from 2012 to 2019. The anatomy and morphology of the aortic root were assessed. "Downsize" strategy was preformed when patients had complex morphology. The clinical outcomes of patients who performed downsize strategy were compared with those received annular sizing strategy. The primary outcome was device success rate, and secondary outcomes included Valve Academic Research Consortium-3 clinical outcomes variables based on 1-year follow-up.
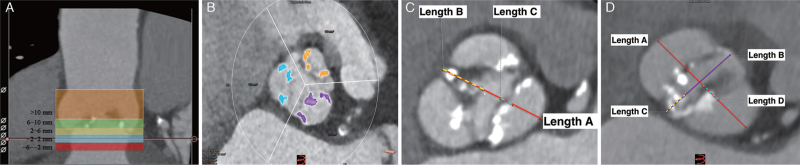
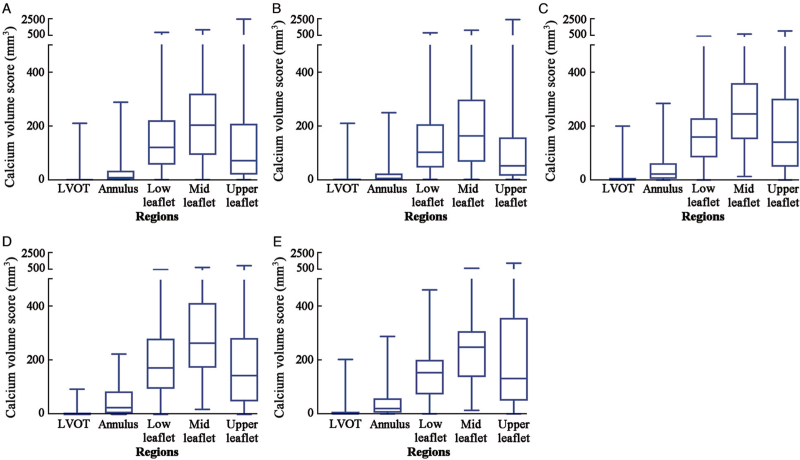
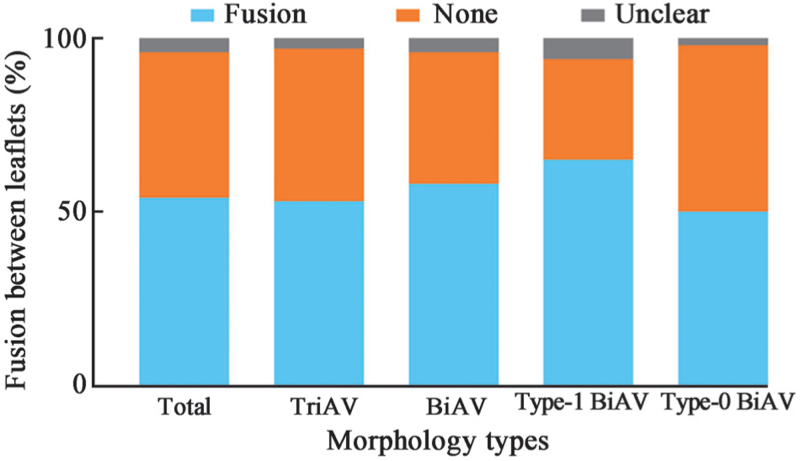
Results: A total of 293 patients were enrolled. Among them, 95 patients (32.4%) had bicuspid aortic valve. The calcium volume (Hounsfield Unit-850) of aortic root was 449.90 (243.15-782.15) mm 3 . Calcium is distributed mostly on the leaflet level. Downsize strategy was performed in 204 patients (69.6%). Compared with the patients who performed annular sizing strategy, those received downsize strategy achieved a similar device success rate (82.0% [73] vs . 83.3% [170], P = 0.79). Aortic valve gradients (downsize strategy group vs . annular sizing group, 11.28 mmHg vs. 11.88 mmHg, P = 0.64) and percentages of patients with moderate or severe paravalvular regurgitation 2.0% (4/204) vs . 4.5% (4/89), P = 0.21) were similar in the two groups at 30 days after TAVR. These echocardiographic results were sustainable for one year.
Conclusions: Chinese TAVR patients have more prevalent bicuspid morphology and large calcium volume of aortic root. Calcium is distributed mostly on the leaflet level. Compare with annular sizing strategy, downsize strategy provided a non-inferior device success rate and transcatheter heart valve hemodynamic performance in self-expanding TAVR procedure.
Copyright © 2023 The Chinese Medical Association, produced by Wolters Kluwer, Inc. under the CC-BY-NC-ND license.
Conflict of interest statement
Dr. Walid Ben Ali has received a research grant from Medtronic and Edward LifeSciences. Dr. Thomas Modine serves as a consultant to Abbott, Boston Scientific, Edwards Lifesciences, GE, Medtronic, and MicroPort.
Figures
References
-
- Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, et al. . Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med 2014; 370:1790–1798. doi: 10.1056/NEJMoa1400590. - PubMed
-
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. . Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010; 363:1597–1607. doi: 10.1056/NEJMoa1008232. - PubMed
-
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. . Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med 2011; 364:2187–2198. doi: 10.1056/NEJMoa1103510. - PubMed
-
- Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Sondergaard L, Mumtaz M, et al. . Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med 2017; 376:1321–1331. doi: 10.1056/NEJMoa1700456. - PubMed
-
- Thourani VH, Kodali S, Makkar RR, Herrmann HC, Williams M, Babaliaros V, et al. . Transcatheter aortic valve replacement versus surgical valve replacement in intermediate-risk patients: a propensity score analysis. Lancet 2016; 387:2218–2225. doi: 10.1016/s0140-6736(16)30073-3. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
