

Biological Burden of Adverse Childhood Experiences in Children
- PMID: 36728584
- PMCID: PMC9930178
- DOI: 10.1097/PSY.0000000000001167
Biological Burden of Adverse Childhood Experiences in Children
Abstract
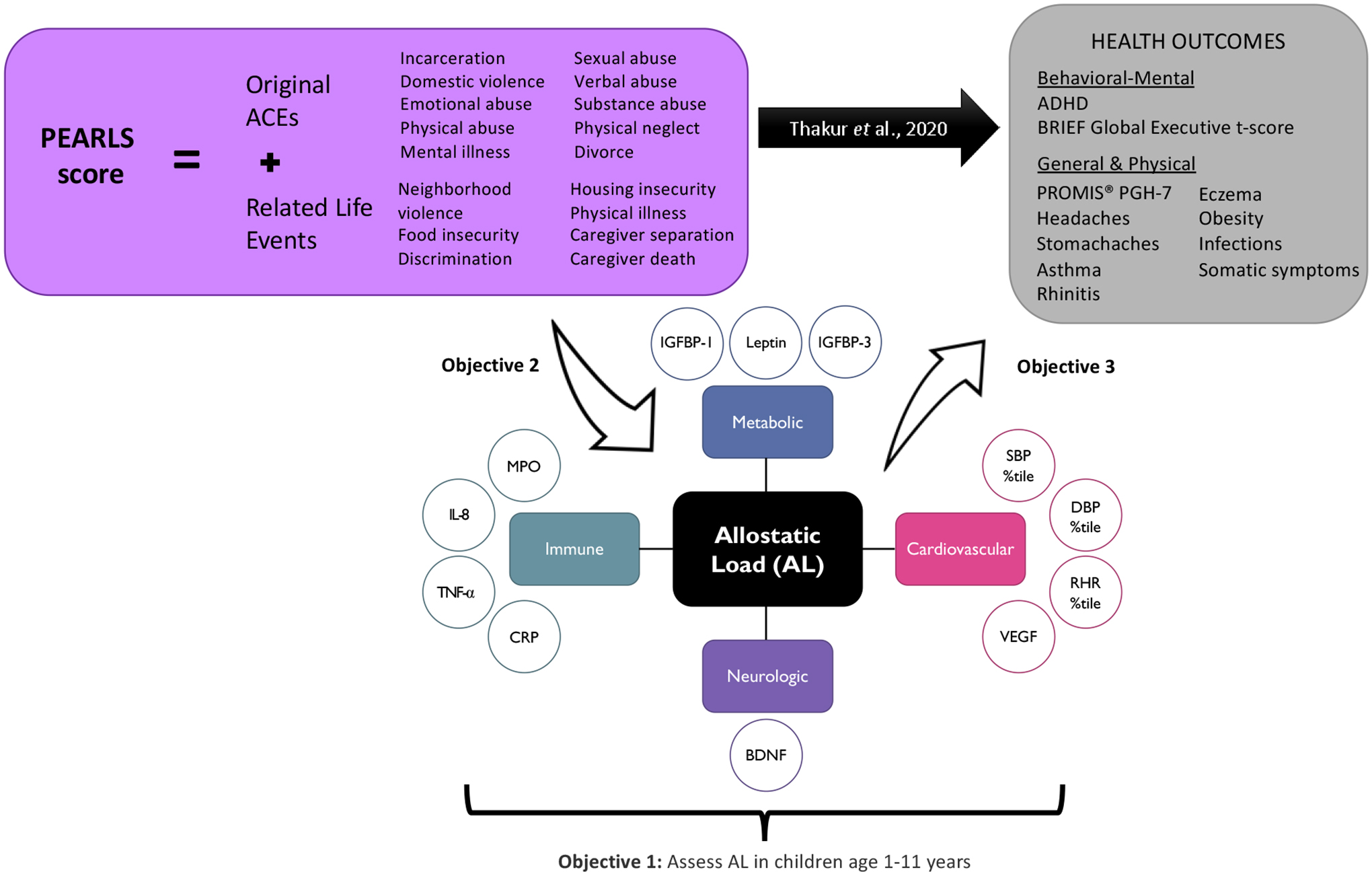
Objective: This study aimed to examine relationships between adverse childhood experiences (ACEs) and related life events and allostatic load (AL)-"wear and tear" from chronic stress-in a pediatric population.
Methods: Children were screened with the PEdiatric ACEs and Related Life Event Screener (PEARLS) tool, a 17-item questionnaire capturing experiences of abuse, neglect, household challenges, and related life events. Biological data were available for 207 participants, and AL was operationalized using clinical or empirical cutoff points across 4 physiological systems (i.e., cardiac, metabolic, inflammatory, neurologic). Covariate-adjusted multivariable regression models were used to examine associations between AL with adversity and health.
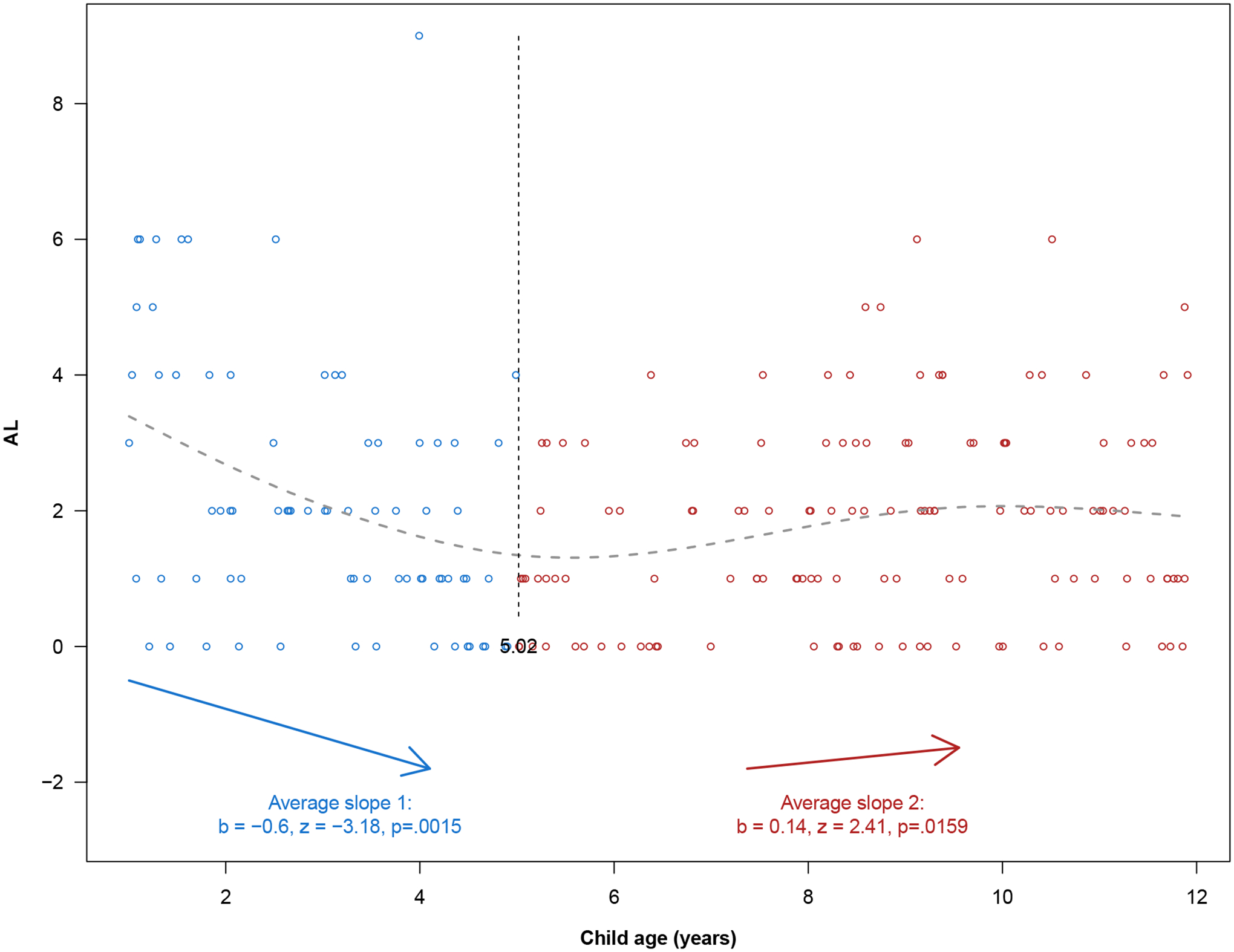
Results: Children (mean age = 6.5 years, range = 1-11 years) had an average AL score of 1.9 (standard deviation = 1.7), and a U-shaped relationship was observed with child's age. Continuous PEARLS and original ACE scores were not associated with AL. However, children with a reported PEARLS score of 1 to 2 or original ACEs score of 1 to 3 had 1.5 (incidence rate ratio [IRR] = 1.50, 95% confidence interval [CI] = 1.09-2.08) and 1.4 (IRR = 1.41, 95% CI = 1.08-1.84) times greater AL, respectively, compared with participants with none reported. In secondary analyses, caregiver mental illness was associated with higher child AL (adjusted IRR = 1.27, 95% CI = 1.01-1.58). AL was also associated with poorer perceived child general health (adjusted β = -0.87, 95% CI = -1.58 to -0.15) and greater odds of child obesity (adjusted odds ratio = 1.51, 95% CI = 1.23-1.89).
Conclusions: Measuring AL in a pediatric population requires careful consideration of age. Higher AL was associated with a greater number of reported adversities and worse child health.
Copyright © 2022 by the American Psychosomatic Society.
Figures
References
-
- Felitti, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine. 1998;14:245–58. - PubMed
-
- Flaherty EG, Thompson R, Litrownik AJ, Theodore A, English DJ, Black MM, Wike T, Whimper L, Runyan DK, Dubowitz H. Effect of early childhood adversity on child health. Archives of Pediatrics & Adolescent Medicine. 2006;160:1232–38. - PubMed
-
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, Jones L, Dunne MP. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet. Public Health. 2017;2:e356–66. - PubMed
