

A Randomized Trial of Intra-articular Injection Therapy for Knee Osteoarthritis
- PMID: 36728848
- PMCID: PMC10090303
- DOI: 10.1097/RLI.0000000000000942
A Randomized Trial of Intra-articular Injection Therapy for Knee Osteoarthritis
Abstract
Background: Intra-articular injections are widely used for conservative treatment of knee osteoarthritis (OA). However, rigorous data are lacking regarding the comparative therapeutic effectiveness of these injections.
Purpose: The aim of this study was to compare clinical outcomes after intra-articular injections of glucocorticoid, hyaluronic acid, platelet-rich plasma (PRP), or placebo in patients with mild or moderate OA of the knee.
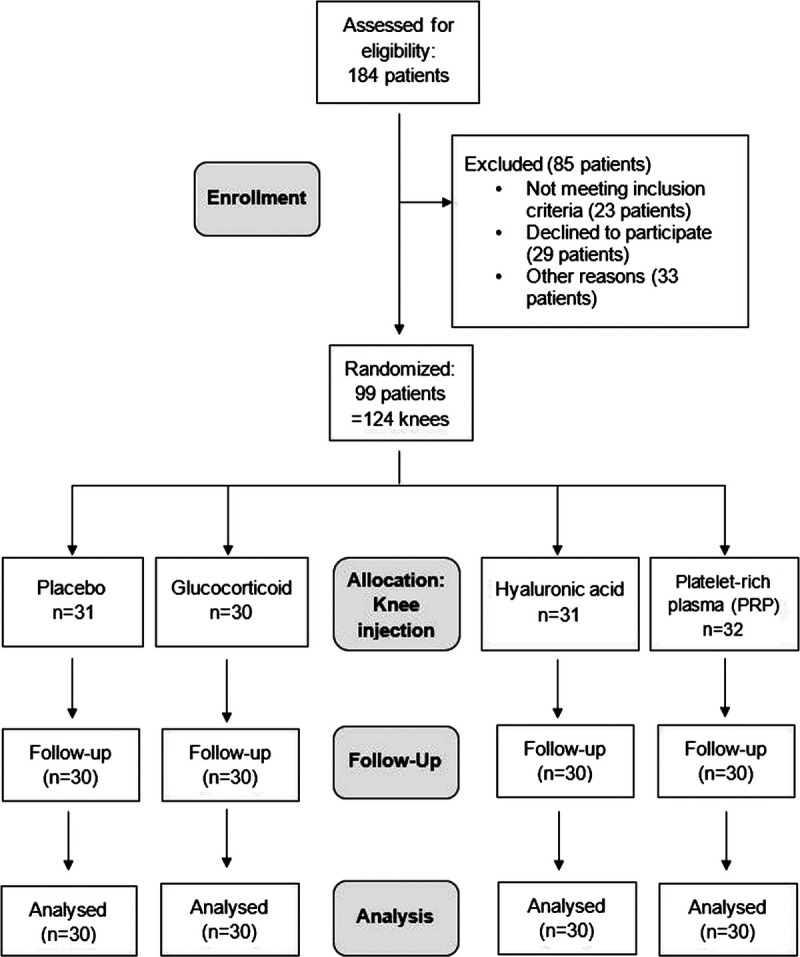
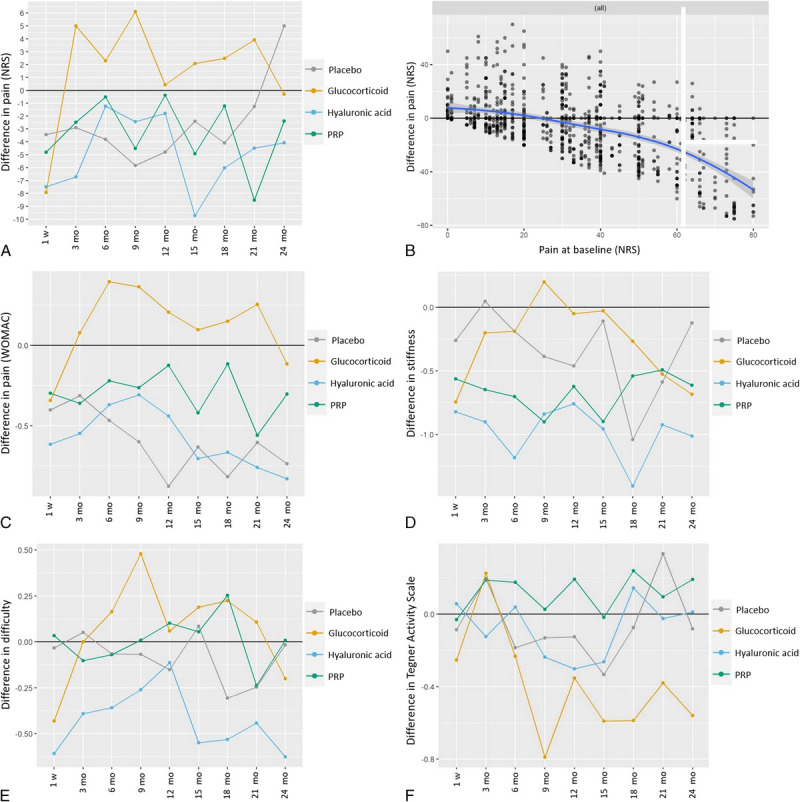
Materials and methods: In a double-blinded, placebo-controlled, single-center trial, we randomly assigned knees with early- to middle-stage knee OA (Kellgren-Lawrence grade 1-3) to an intra-articular injection with one of these substances: glucocorticoid, hyaluronic acid, PRP, or placebo. Primary outcome was pain reduction within 6 months after the injection, assessed with the numeric rating scale (NRS; range, 0-100). Secondary outcome parameters included WOMAC scores, Tegner Activity Scale, knee mobility, and adverse events. Finally, a linear mixed-effects model was calculated and corrected for possible patient and covariate effects.
Results: One hundred twenty knees (30 knees per treatment group) in 95 patients (41 female) were included in the final analysis. The median age of patients was 60 years (interquartile range, 54.0-68.0). There was no evidence that the drug effects of primary and secondary outcome parameters differed over time. The median pain at baseline was 32.5 (interquartile range, 15.00-50.00) on NRS. The changes in pain level during the first 6 months compared with baseline were small (within ±5 points on NRS), whereas the intrapatient variability was large between -20 and +20 points. Secondary outcome parameters did not differ significantly among the groups. Kellgren-Lawrence grade did not have a statistically significant effect on pain reduction ( P = 0.61).
Conclusions: There is no evidence that knee injections with glucocorticoid, PRP, or hyaluronic acid have superior short- or long-term effects in patients with low pain level at baseline and early- to middle-stage knee OA when compared with placebo.
Trial registration: ClinicalTrials.gov NCT02776514.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Conflicts of interest and sources of funding: None of the authors has anything to disclose. Data generated or analyzed during the study and the study protocol are available from the corresponding author by request.
Figures
References
-
- Sharma L. Osteoarthritis of the knee. N Engl J Med. 2021;384:51–59. - PubMed
-
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–1759. - PubMed
-
- Safiri S Kolahi AA Cross M, et al. Prevalence, incidence, and years lived with disability due to gout and its attributable risk factors for 195 countries and territories 1990–2017: a systematic analysis of the global burden of disease study 2017. Arthritis Rheumatol. 2020;72:1916–1927. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
