

The diagnostic challenge of non-traumatic bladder rupture: a pictorial essay
- PMID: 36729190
- PMCID: PMC10313837
- DOI: 10.1007/s11604-023-01395-1
The diagnostic challenge of non-traumatic bladder rupture: a pictorial essay
Abstract
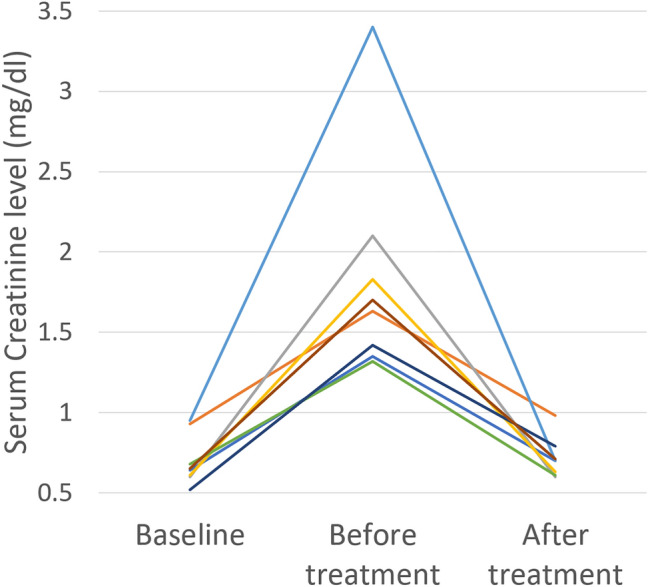
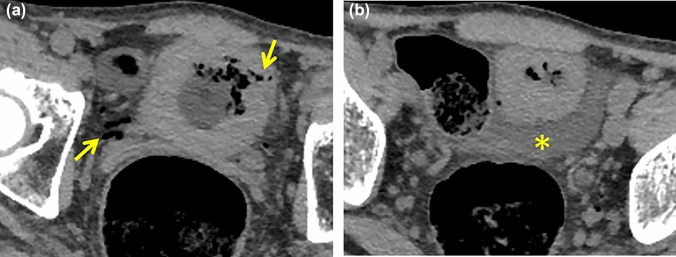
Non-traumatic bladder rupture (NTBR) is relative rare pathology including spontaneous rupture and iatrogenic injury. As increasing the medical intervention for the pelvic malignancy or elderly population, NTBR will be encountered more frequently. There are few previous studies summarizing the imaging features of NTBR. We reviewed imaging characteristics of 18 previous cases of NTBR experienced. In addition, 3 presentative cases that can be a pitfall to differentiate from NTBR. The aim of this article is to clarify the key CT findings of NTBR and its pitfalls.
Keywords: Bladder rupture; Computed tomography; Non-traumatic; Pseudo-renal failure.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
