

Cost-effectiveness of Aflibercept Monotherapy vs Bevacizumab First Followed by Aflibercept If Needed for Diabetic Macular Edema
- PMID: 36729431
- PMCID: PMC9896372
- DOI: 10.1001/jamaophthalmol.2022.6142
Cost-effectiveness of Aflibercept Monotherapy vs Bevacizumab First Followed by Aflibercept If Needed for Diabetic Macular Edema
Abstract
Importance: The DRCR Retina Network Protocol AC showed no significant difference in visual acuity outcomes over 2 years between treatment with aflibercept monotherapy and bevacizumab first with switching to aflibercept for suboptimal response in treating diabetic macular edema (DME). Understanding the estimated cost and cost-effectiveness of these approaches is important.
Objective: To evaluate the cost and cost-effectiveness of aflibercept monotherapy vs bevacizumab-first strategies for DME treatment.
Design, setting, and participants: This economic evaluation was a preplanned secondary analysis of a US randomized clinical trial of participants aged 18 years or older with center-involved DME and best-corrected visual acuity of 20/50 to 20/320 enrolled from December 15, 2017, through November 25, 2019.
Interventions: Aflibercept monotherapy or bevacizumab first, switching to aflibercept in eyes with protocol-defined suboptimal response.
Main outcomes and measures: Between February and July 2022, the incremental cost-effectiveness ratio (ICER) in cost per quality-adjusted life-year (QALY) over 2 years was assessed. Efficacy and resource utilization data from the randomized clinical trial were used with health utility mapping from the literature and Medicare unit costs.
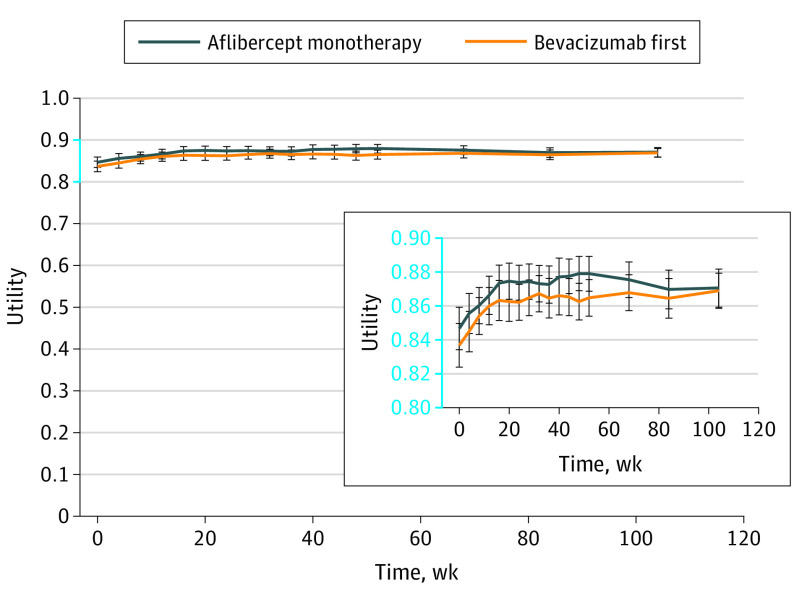
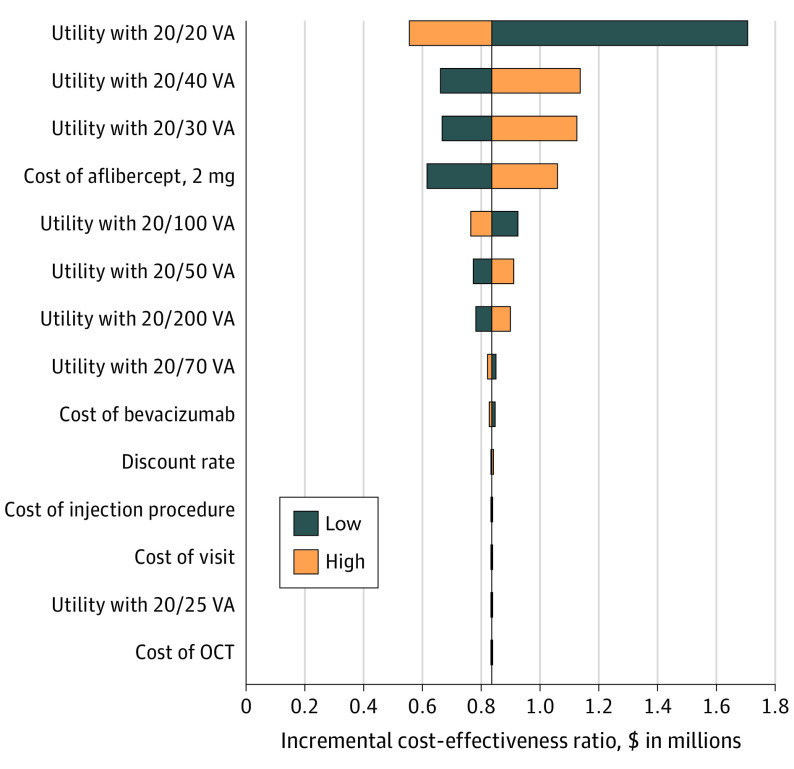
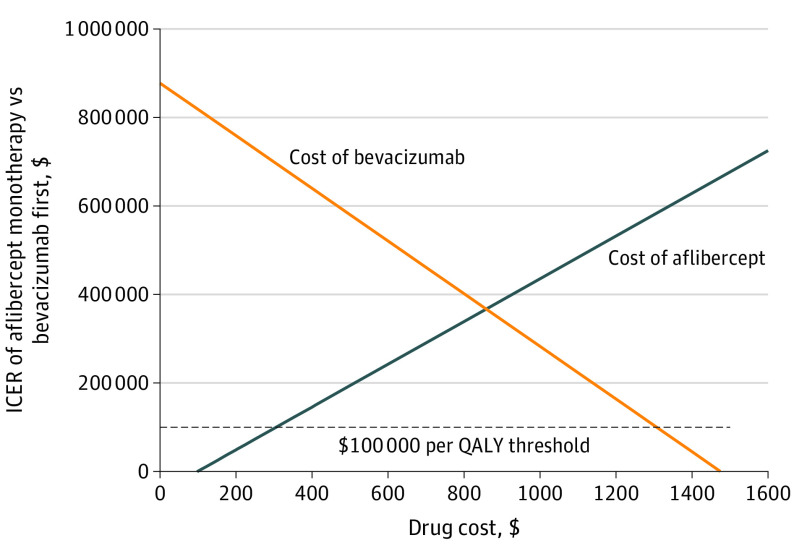
Results: This study included 228 participants (median age, 62 [range, 34-91 years; 116 [51%] female and 112 [49%] male; 44 [19%] Black or African American, 60 [26%] Hispanic or Latino, and 117 [51%] White) with 1 study eye. The aflibercept monotherapy group included 116 participants, and the bevacizumab-first group included 112, of whom 62.5% were eventually switched to aflibercept. Over 2 years, the cost of aflibercept monotherapy was $26 504 (95% CI, $24 796-$28 212) vs $13 929 (95% CI, $11 984-$15 874) for the bevacizumab-first group, a difference of $12 575 (95% CI, $9987-$15 163). The aflibercept monotherapy group gained 0.015 (95% CI, -0.011 to 0.041) QALYs using the better-seeing eye and had an ICER of $837 077 per QALY gained compared with the bevacizumab-first group. Aflibercept could be cost-effective with an ICER of $100 000 per QALY if the price per dose were $305 or less or the price of bevacizumab was $1307 per dose or more.
Conclusions and relevance: Variability in individual needs will influence clinician and patient decisions about how to treat specific eyes with DME. While the bevacizumab-first group costs still averaged approximately $14 000 over 2 years, this approach, as used in this study, may confer substantial cost savings on a societal level without sacrificing visual acuity gains over 2 years compared with aflibercept monotherapy.
Conflict of interest statement
Figures
References
-
- American Society of Retina Specialists. Preferences and Trends (PAT) survey. 2021. Accessed August 15, 2022. https://www.asrs.org/asrs-community/pat-survey/pat-survey
-
- Wells JA, Glassman AR, Ayala AR, et al. ; Diabetic Retinopathy Clinical Research Network . Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123(6):1351-1359. doi: 10.1016/j.ophtha.2016.02.022 - DOI - PMC - PubMed
-
- Centers for Medicare & Medicaid Services. 2022 ASP drug pricing files. 2022. Accessed February 24, 2022. https://www.cms.gov/medicare/medicare-part-b-drug-average-sales-price/20...
-
- Centers for Medicare & Medicaid Services. RVU22A. 2022. Accessed August 15, 2022. https://www.cms.gov/medicaremedicare-fee-service-paymentphysicianfeesche...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
