

Breast Cancer Diagnosis, Treatment, and Outcomes of Patients From Sex and Gender Minority Groups
- PMID: 36729432
- PMCID: PMC9896373
- DOI: 10.1001/jamaoncol.2022.7146
Breast Cancer Diagnosis, Treatment, and Outcomes of Patients From Sex and Gender Minority Groups
Abstract
Importance: Sexual orientation and gender identity data are not collected by most hospitals or cancer registries; thus, little is known about the quality of breast cancer treatment for patients from sex and gender minority (SGM) groups.
Objective: To evaluate the quality of breast cancer treatment and recurrence outcomes for patients from SGM groups compared with cisgender heterosexual patients.
Design, setting, and participants: Exposure-matched retrospective case-control study of 92 patients from SGM groups treated at an academic medical center from January 1, 2008, to January 1, 2022, matched to cisgender heterosexual patients with breast cancer by year of diagnosis, age, tumor stage, estrogen receptor status, and ERBB2 (HER2) status.
Main outcomes and measures: Patient demographic and clinical characteristics, as well as treatment quality, as measured by missed guideline-based breast cancer screening, appropriate referral for genetic counseling and testing, mastectomy vs lumpectomy, receipt of chest reconstruction, adjuvant radiation therapy after lumpectomy, neoadjuvant chemotherapy for stage III disease, antiestrogen therapy for at least 5 years for estrogen receptor-positive disease, ERBB2-directed therapy for ERBB2-positive disease, patient refusal of an oncologist-recommended treatment, time from symptom onset to tissue diagnosis, time from diagnosis to first treatment, and time from breast cancer diagnosis to first recurrence. Results were adjusted for multiple hypothesis testing. Compared with cisgender heterosexual patients, those from SGM groups were hypothesized to have disparities in 1 or more of these quality metrics.
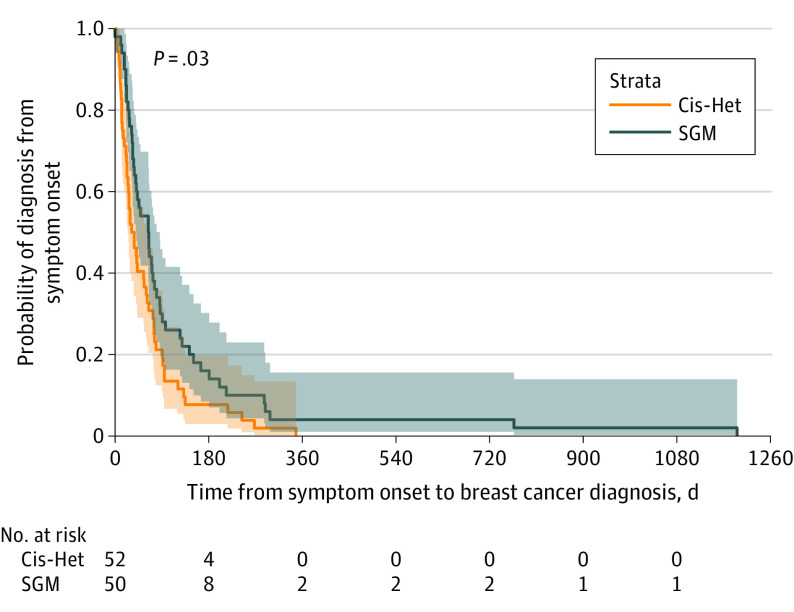
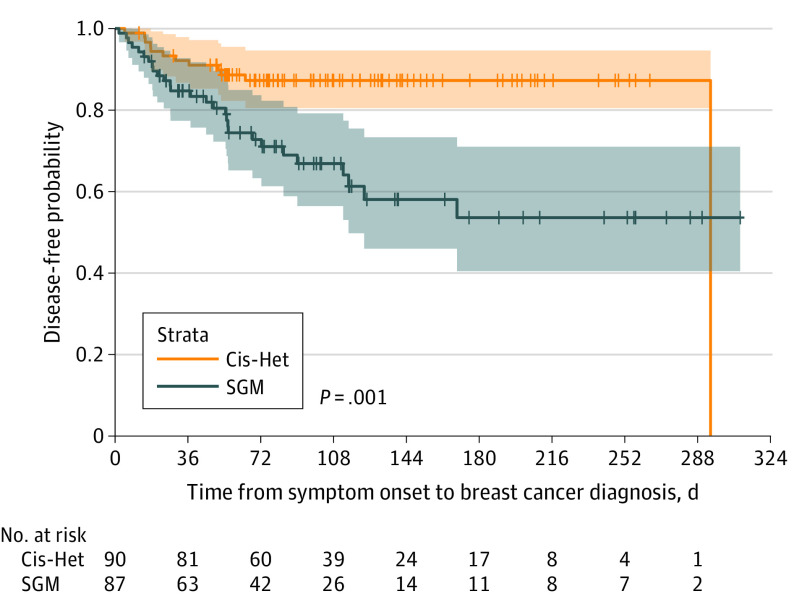
Results: Ninety-two patients from SGM groups were matched to 92 cisgender heterosexual patients (n = 184). The median age at diagnosis for all patients was 49 years (IQR, 43-56 years); 74 were lesbian (80%), 12 were bisexual (13%), and 6 were transgender (6%). Compared with cisgender heterosexual patients, those from SGM groups experienced a delay in time from symptom onset to diagnosis (median time to diagnosis, 34 vs 64 days; multivariable adjusted hazard ratio, 0.65; 95% CI, 0.42-0.99; P = .04), were more likely to decline an oncologist-recommended treatment modality (35 [38%] vs 18 [20%]; multivariable adjusted odds ratio, 2.27; 95% CI, 1.09-4.74; P = .03), and were more likely to experience a breast cancer recurrence (multivariable adjusted hazard ratio, 3.07; 95% CI, 1.56-6.03; P = .001).
Conclusions and relevance: This study found that among patients with breast cancer, those from SGM groups experienced delayed diagnosis, with faster recurrence at a 3-fold higher rate compared with cisgender heterosexual patients. These results suggest disparities in the care of patients from SGM groups and warrant further study to inform interventions.
Conflict of interest statement
Figures
Comment in
-
Breast cancer disparities among sexual and gender minority populations.Transl Cancer Res. 2023 Aug 31;12(8):2219-2223. doi: 10.21037/tcr-23-623. Epub 2023 Aug 3. Transl Cancer Res. 2023. PMID: 37701114 Free PMC article. No abstract available.
-
Breast cancer diagnosis, treatment, and outcomes of patients from sex and gender minority groups.Transl Cancer Res. 2023 Oct 31;12(10):2458-2460. doi: 10.21037/tcr-23-833. Epub 2023 Sep 25. Transl Cancer Res. 2023. PMID: 37969366 Free PMC article. No abstract available.
References
-
- Schabath MB, Blackburn CA, Sutter ME, et al. National Survey of Oncologists at National Cancer Institute–designated comprehensive cancer centers: attitudes, knowledge, and practice behaviors about LGBTQ patients with cancer. J Clin Oncol. 2019;37(7):547-558. doi: 10.1200/JCO.18.00551 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
