

Automated In Vivo High-Resolution Imaging to Detect Human Papillomavirus-Associated Anal Precancer in Persons Living With HIV
- PMID: 36729506
- PMCID: PMC9944690
- DOI: 10.14309/ctg.0000000000000558
Automated In Vivo High-Resolution Imaging to Detect Human Papillomavirus-Associated Anal Precancer in Persons Living With HIV
Abstract
Introduction: In the United States, the effectiveness of anal cancer screening programs has been limited by a lack of trained professionals proficient in high-resolution anoscopy (HRA) and a high patient lost-to-follow-up rate between diagnosis and treatment. Simplifying anal intraepithelial neoplasia grade 2 or more severe (AIN 2+) detection could radically improve the access and efficiency of anal cancer prevention. Novel optical imaging providing point-of-care diagnoses could substantially improve existing HRA and histology-based diagnosis. This work aims to demonstrate the potential of high-resolution microendoscopy (HRME) coupled with a novel machine learning algorithm for the automated, in vivo diagnosis of anal precancer.
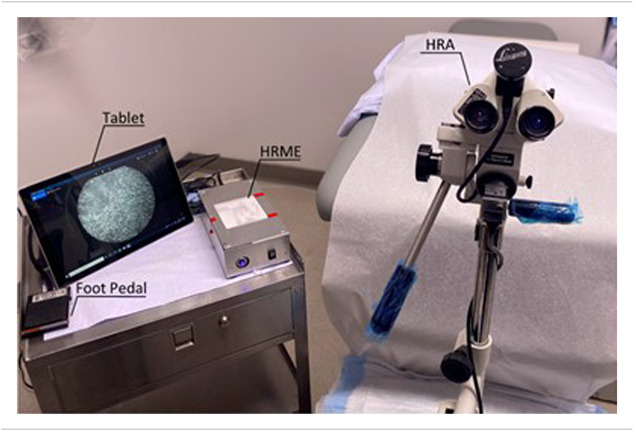
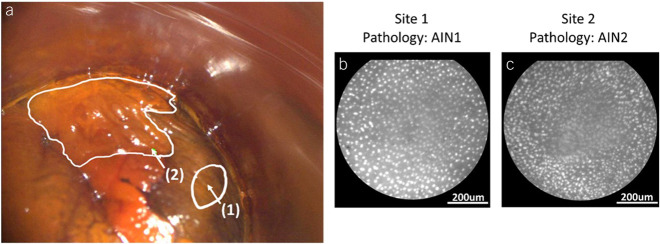
Methods: The HRME, a fiber-optic fluorescence microscope, was used to capture real-time images of anal squamous epithelial nuclei. Nuclear staining is achieved using 0.01% wt/vol proflavine, a topical contrast agent. HRME images were analyzed by a multitask deep learning network (MTN) that computed the probability of AIN 2+ for each HRME image.
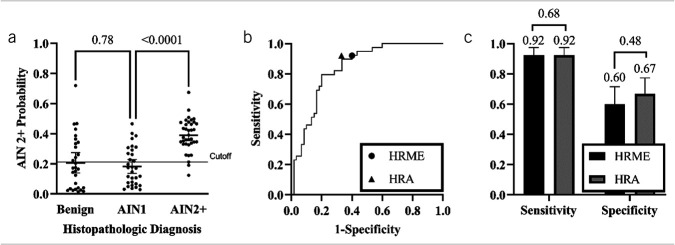
Results: The study accrued data from 77 people living with HIV. The MTN achieved an area under the receiver operating curve of 0.84 for detection of AIN 2+. At the AIN 2+ probability cutoff of 0.212, the MTN achieved comparable performance to expert HRA impression with a sensitivity of 0.92 ( P = 0.68) and specificity of 0.60 ( P = 0.48) when using histopathology as the gold standard.
Discussion: When used in combination with HRA, this system could facilitate more selective biopsies and promote same-day AIN2+ treatment options by enabling real-time diagnosis.
Trial registration: ClinicalTrials.gov NCT04563754.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med 2011;365(17):1576–85. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
