

Biomarker Data from the Phase III KATHERINE Study of Adjuvant T-DM1 versus Trastuzumab for Residual Invasive Disease after Neoadjuvant Therapy for HER2-Positive Breast Cancer
- PMID: 36730339
- PMCID: PMC10102844
- DOI: 10.1158/1078-0432.CCR-22-1989
Biomarker Data from the Phase III KATHERINE Study of Adjuvant T-DM1 versus Trastuzumab for Residual Invasive Disease after Neoadjuvant Therapy for HER2-Positive Breast Cancer
Abstract
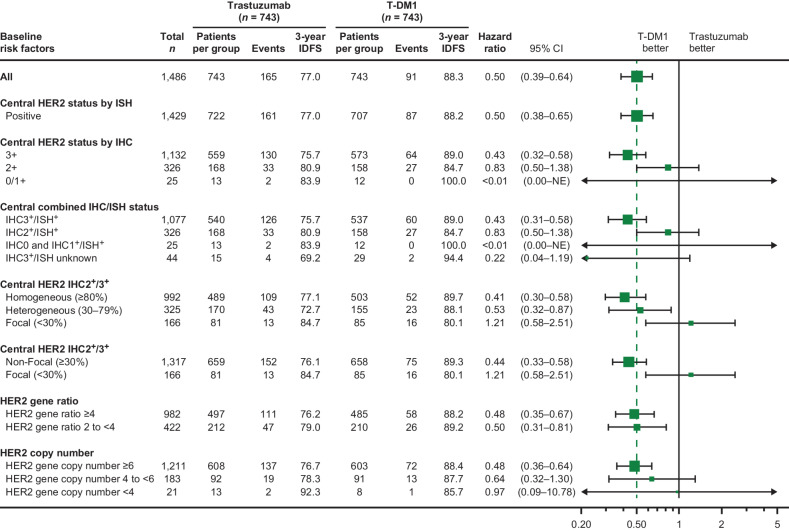
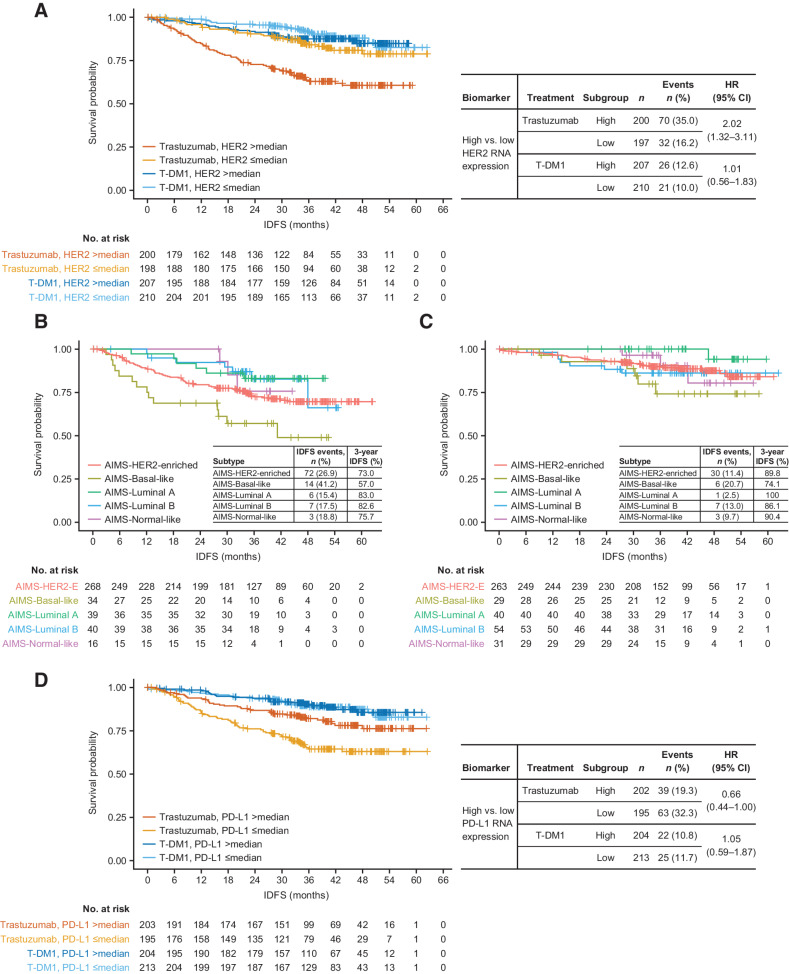
Purpose: In KATHERINE, adjuvant T-DM1 reduced risk of disease recurrence or death by 50% compared with trastuzumab in patients with residual invasive breast cancer after neoadjuvant therapy (NAT) comprised of HER2-targeted therapy and chemotherapy. This analysis aimed to identify biomarkers of response and differences in biomarker expression before and after NAT.
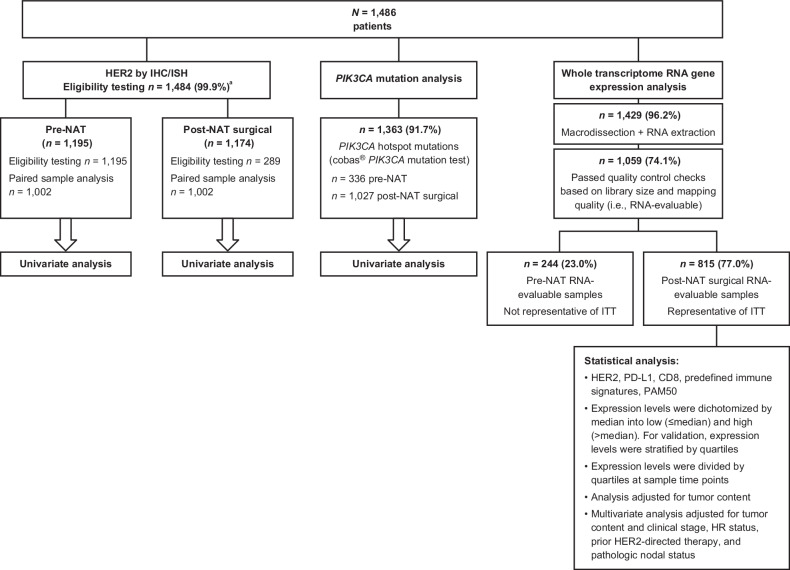
Experimental design: Exploratory analyses investigated the relationship between invasive disease-free survival (IDFS) and HER2 protein expression/gene amplification, PIK3CA hotspot mutations, and gene expression of HER2, PD-L1, CD8, predefined immune signatures, and Prediction Analysis of Microarray 50 intrinsic molecular subtypes, classified by Absolute Intrinsic Molecular Subtyping. HER2 expression on paired pre- and post-NAT samples was examined.
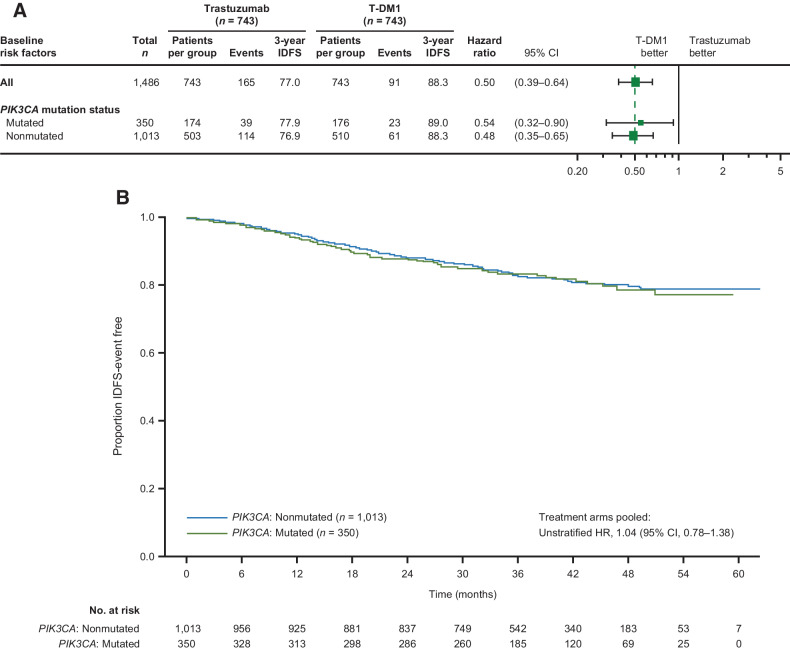
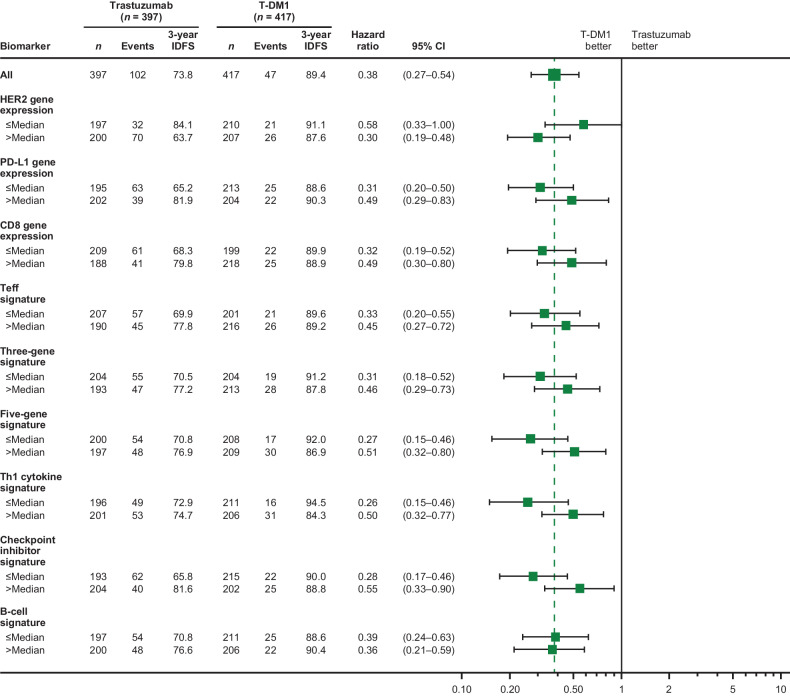
Results: T-DM1 appeared to improve IDFS versus trastuzumab across most biomarker subgroups, except the HER2 focal expression subgroup. High versus low HER2 gene expression in residual disease was associated with worse outcomes with trastuzumab [HR, 2.02; 95% confidence interval (CI), 1.32-3.11], but IDFS with T-DM1 was independent of HER2 expression level (HR, 1.01; 95% CI, 0.56-1.83). Low PD-L1 gene expression in residual disease was associated with worse outcomes with trastuzumab (HR, 0.66; 95% CI, 0.44-1.00), but not T-DM1 (HR, 1.05; 95% CI, 0.59-1.87). PIK3CA mutations were not prognostic. Increased variability in HER2 expression was observed in post-NAT versus paired pre-NAT samples.
Conclusions: T-DM1 appears to overcome HER2 resistance. T-DM1 benefit does not appear dependent on immune activation, but these results do not rule out an influence of the tumor immune microenvironment on the degree of response.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Untch M, Fasching PA, Konecny GE, Hasmüller S, Lebeau A, Kreienberg R, et al. Pathologic complete response after neoadjuvant chemotherapy plus trastuzumab predicts favorable survival in human epidermal growth factor receptor 2–overexpressing breast cancer: results from the TECHNO trial of the AGO and GBG study groups. J Clin Oncol 2011;29:3351–7. - PubMed
-
- de Azambuja E, Holmes AP, Piccart-Gebhart M, Holmes E, Cosimo SD, Swaby RF, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): survival outcomes of a randomised, open-label, multicentre, phase 3 trial and their association with pathological complete response. Lancet Oncol 2014;15:1137–46. - PubMed
-
- Gianni L, Eiermann W, Semiglazov V, Lluch A, Tjulandin S, Zambetti M, et al. Neoadjuvant and adjuvant trastuzumab in patients with HER2-positive locally advanced breast cancer (NOAH): follow-up of a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet Oncol 2014;15:640–7. - PubMed
-
- Schneeweiss A, Chia S, Hickish T, Harvey V, Eniu A, Waldron-Lynch M, et al. Long-term efficacy analysis of the randomised, phase II TRYPHAENA cardiac safety study: evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer. Eur J Cancer 2018;89:27–35. - PubMed
-
- von Minckwitz G, Huang C-S, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med 2019;380:617–28. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
