

Index Surgery Cost of Fluoroscopic Freehand Versus Robotic-Assisted Pedicle Screw Placement in Lumbar Instrumentation: An Age, Sex, and Approach-Matched Cohort Comparison
- PMID: 36732310
- PMCID: PMC9722569
- DOI: 10.5435/JAAOSGlobal-D-22-00137
Index Surgery Cost of Fluoroscopic Freehand Versus Robotic-Assisted Pedicle Screw Placement in Lumbar Instrumentation: An Age, Sex, and Approach-Matched Cohort Comparison
Abstract
Background: Spine surgery costs are notoriously high, and there are already criticisms and concerns over the economic effects. There is no consensus on cost variation with robot-assisted spine fusion (rLF) compared with a manual fluoroscopic freehand (fLF) approach. This study looks to compare the early costs between the robotic method and the freehand method in lumbar spine fusion.
Methods: rLFs by one spine surgeon were age, sex, and approach-matched to fLF procedures by another spine surgeon. Variable direct costs, readmissions, and revision surgeries within 90 days were reviewed and compared.
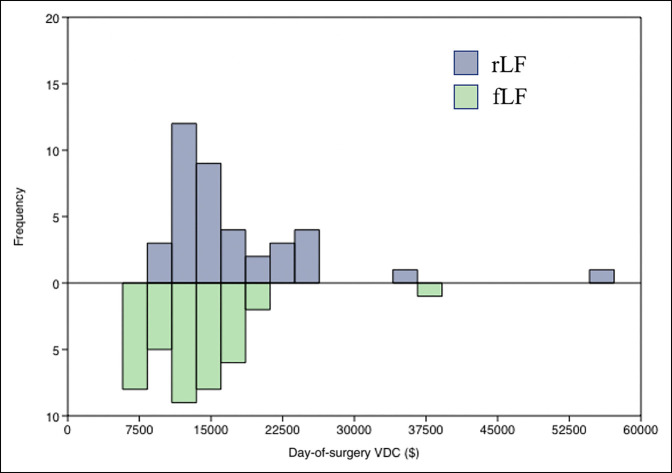
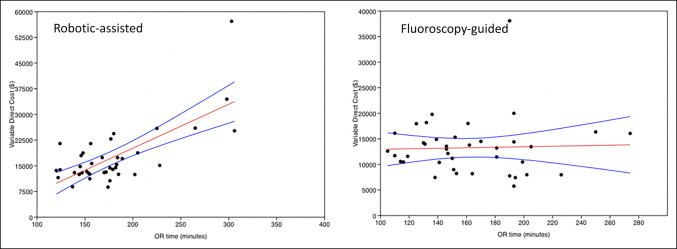
Results: Thirty-nine rLFs were matched to 39 fLF procedures. No significant differences were observed in clinical outcomes. rLF had higher total encounter costs (P < 0.001) and day-of-surgery costs (P = 0.005). Increased costs were mostly because of increased supply cost (0.0183) and operating room time cost (P < 0.001). Linear regression showed a positive relationship with operating room time and cost in rLF (P < 0.001).
Conclusion: rLF is associated with a higher index surgery cost. The main factor driving increased cost is supply costs, with other variables too small in difference to make a notable financial effect. rLF will become more common, and other institutions may need to take a closer financial look at this more novel instrumentation before adoption.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Orthopaedic Surgeons.
Conflict of interest statement
Dr. Khalil or an immediate family member has received royalties from Camber Spine; is a member of a speakers’ bureau or has made paid presentations on behalf of Camber Spine, Centinel Spine, Johnson & Johnson, Medtronic, Relievant Medsystems, and Stryker; serves as a paid consultant to Camber Spine, Centinel Spine, Medtronic, Relievant Medsystems, SI Bone, and Stryker; has stock or stock options held in Johnson & Johnson, Medtronic, and Nuvasive; has received research support from Centinel Spine, Fziomed, Innovative Surgical Designs, Johnson & Johnson, Limiflex, Medtronic, Relievant, and Stryker; and serves as a board or committee member of the American Academy of Orthopaedic Surgeons; serves on the editorial or governing board of the Journal of the American Academy of Orthopaedic Surgeons. Dr. Park or an immediate family member serves as a paid consultant to Arthrex, Kuros, Orthofix, Solco, Stryker, and Theramatrix; has stock or stock options held in Johnson and Johnson, Stryker, and Surgalign; serves as a board or committee member of the American Academy of Orthopaedic Surgeons and the Cervical Spine Research Society; and serves on the editorial or governing board of Orthoinfo. None of the following authors or any immediate family member has received anything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject of this article: Ezeokoli, Pfennig, John, and Gupta.
Figures
References
-
- Wray S, Mimran R, Vadapalli S, Shetye SS, McGilvray KC, Puttlitz CM: Pedicle screw placement in the lumbar spine: Effect of trajectory and screw design on acute biomechanical purchase. J Neurosurg Spine 2015;22:503-510. - PubMed
-
- Molliqaj G, Schatlo B, Alaid A, et al. : Accuracy of robot-guided versus freehand fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery. Neurosurg Focus 2017;42:E14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
