

Patients with isolated REM-sleep behavior disorder have elevated levels of alpha-synuclein aggregates in stool
- PMID: 36732520
- PMCID: PMC9895074
- DOI: 10.1038/s41531-023-00458-4
Patients with isolated REM-sleep behavior disorder have elevated levels of alpha-synuclein aggregates in stool
Abstract
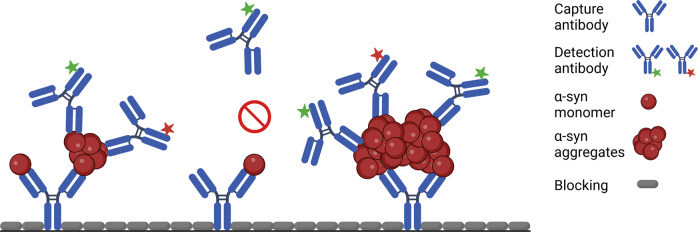
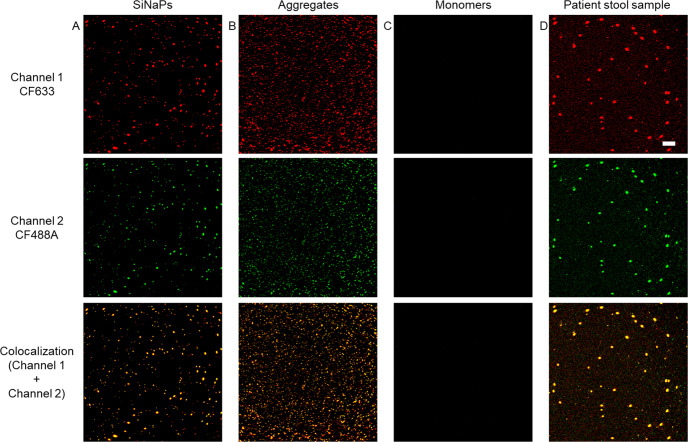
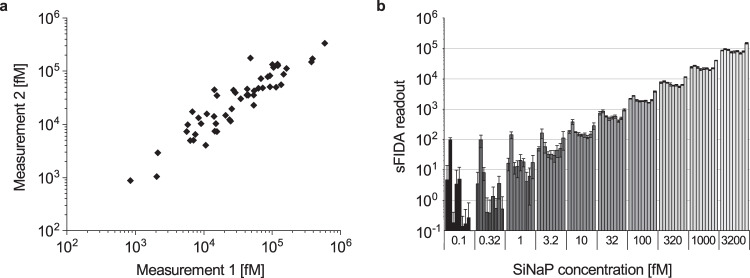
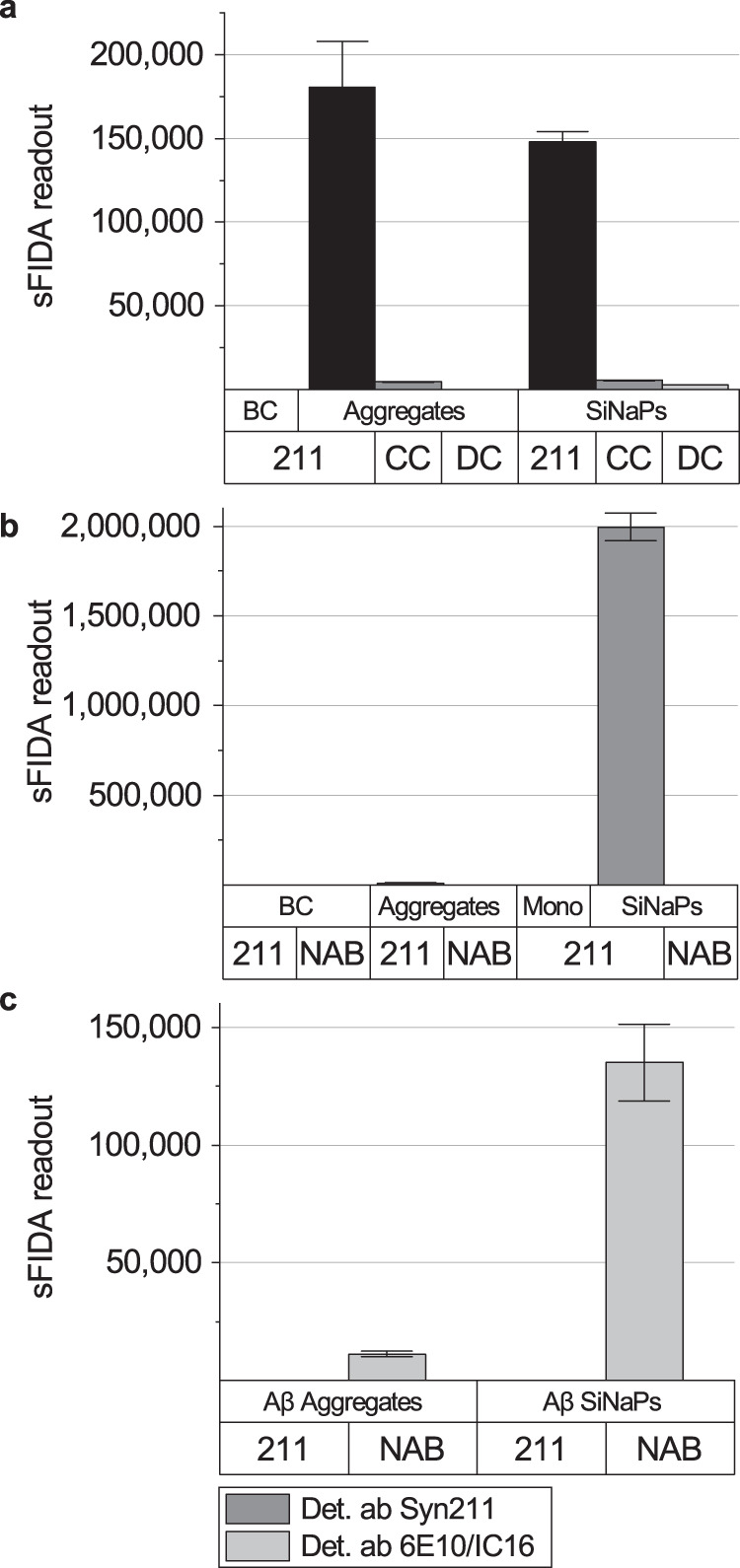
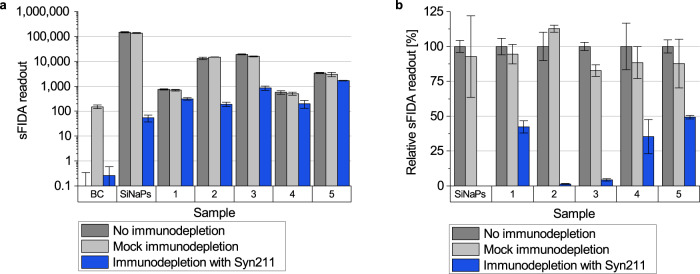
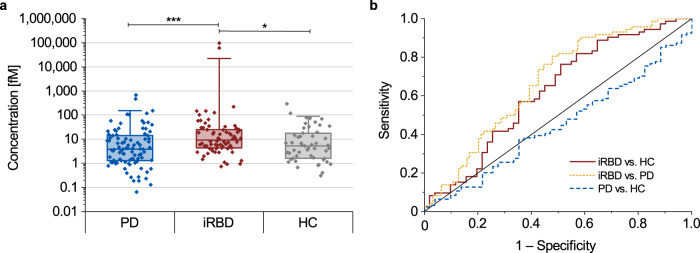
Misfolded and aggregated α-synuclein is a neuropathological hallmark of Parkinson's disease (PD). Thus, α-synuclein aggregates are regarded as a biomarker for the development of diagnostic assays. Quantification of α-synuclein aggregates in body fluids is challenging, and requires highly sensitive and specific assays. Recent studies suggest that α-synuclein aggregates may be shed into stool. We used surface-based fluorescence intensity distribution analysis (sFIDA) to detect and quantify single particles of α-synuclein aggregates in stool of 94 PD patients, 72 isolated rapid eye movement sleep behavior disorder (iRBD) patients, and 51 healthy controls. We measured significantly elevated concentrations of α-synuclein aggregates in stool of iRBD patients versus those of controls (p = 0.024) or PD patients (p < 0.001). Our results show that α-synuclein aggregates are excreted in stool and can be measured using the sFIDA assay, which could support the diagnosis of prodromal synucleinopathies.
© 2023. The Author(s).
Conflict of interest statement
D.W. and O.B. declare no competing non-financial interests but the following competing financial interests: D.W. and O.B. are shareholders of attyloid GmbH. A.S., S.S., A.S., H.J., P.Ö., M.P., L.B., A.C., J.W., T.B., G.R.R., M.S., M.T.B., and G.T. declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
