

Adverse events are not increased by controlled delay in surgery of acute upper extremity fractures
- PMID: 36732558
- PMCID: PMC9894821
- DOI: 10.1038/s41598-023-28921-5
Adverse events are not increased by controlled delay in surgery of acute upper extremity fractures
Abstract
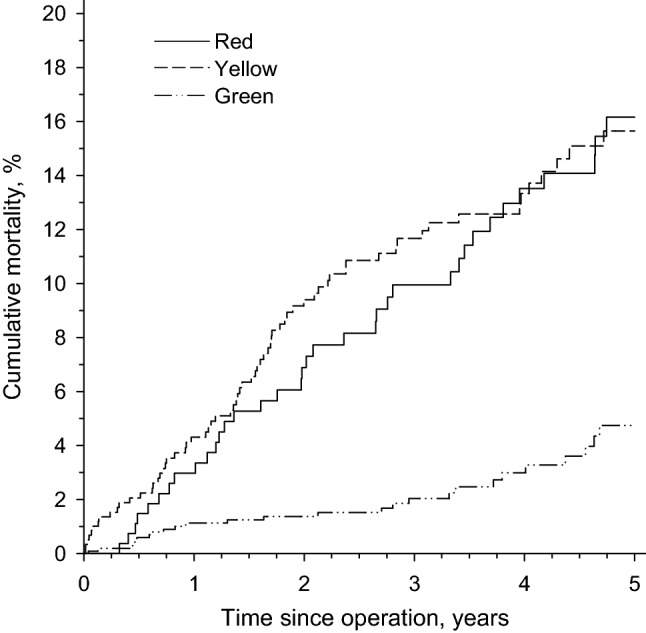
Management of the operative treatment of fractures is challenged by daily variation in patient flow. For upper limb fractures there has recently been an increasing tendency to temporarily discharge the patient to wait for a daytime operation to be performed during the next few days. The objective of this study was to study the safety of controlled delay in surgery. Upper limb fractures (N = 1 944) treated in a level 2 trauma center from 2010 to 2016 were identified and included in this retrospective cohort study with 5-year follow-up. Delay in surgery, inpatient time, readmissions, ED revisits and mortality were analyzed. Depending on the nature of the injury, controlled delay to surgery was implemented. Urgency of surgery was coded as green (2 days to 2 weeks) yellow (8-48 h) or red (less than 8 h). Harms and benefits to the groups were compared. Controlled delay of surgery (median delay of 5 days 7 h) was applied in 1 074 out of 1 944 fractures. The number of revisits to the emergency department (11.1% vs. 17.9-24.1%, p < 0.001) or hospital readmissions for any reason (0.99 per 100 person years in the delayed group vs. 3.74 and 4.35 in the non-delayed groups, p < 0.001) was no higher in patients with delayed (green) compared to those with non-delayed (yellow and red) operations. Inpatient time was significantly lower in the delayed group than other groups (IRR 2.31-3.36, (p < 0.001)). The standardized mortality ratio was 0.83 (CI 0.57-1.22) in the delayed group vs. 1.49 (CI 1.17-1.90) and 1.61 (CI 1.16-2.23) in the non-delayed groups. Controlled delay in upper limb trauma surgery did not lead to increased readmissions or mortality and was associated with reduced inpatient time.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
