

Multimodal deep learning of fundus abnormalities and traditional risk factors for cardiovascular risk prediction
- PMID: 36732671
- PMCID: PMC9894867
- DOI: 10.1038/s41746-023-00748-4
Multimodal deep learning of fundus abnormalities and traditional risk factors for cardiovascular risk prediction
Abstract
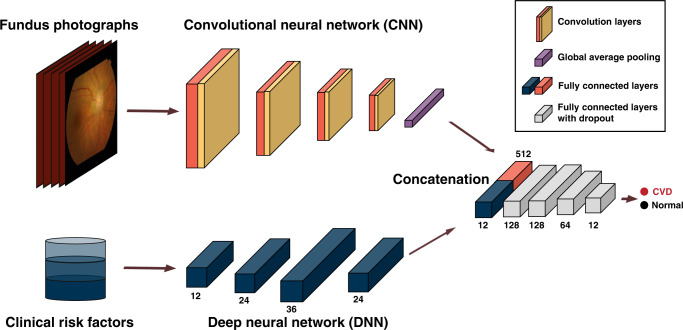
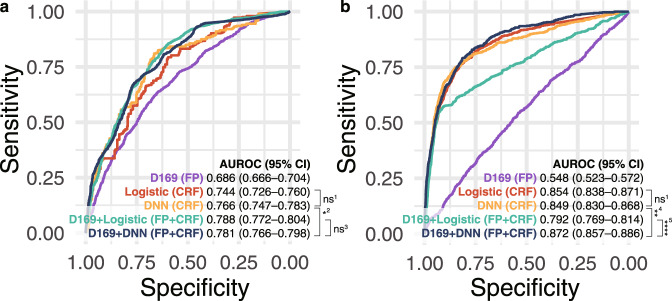
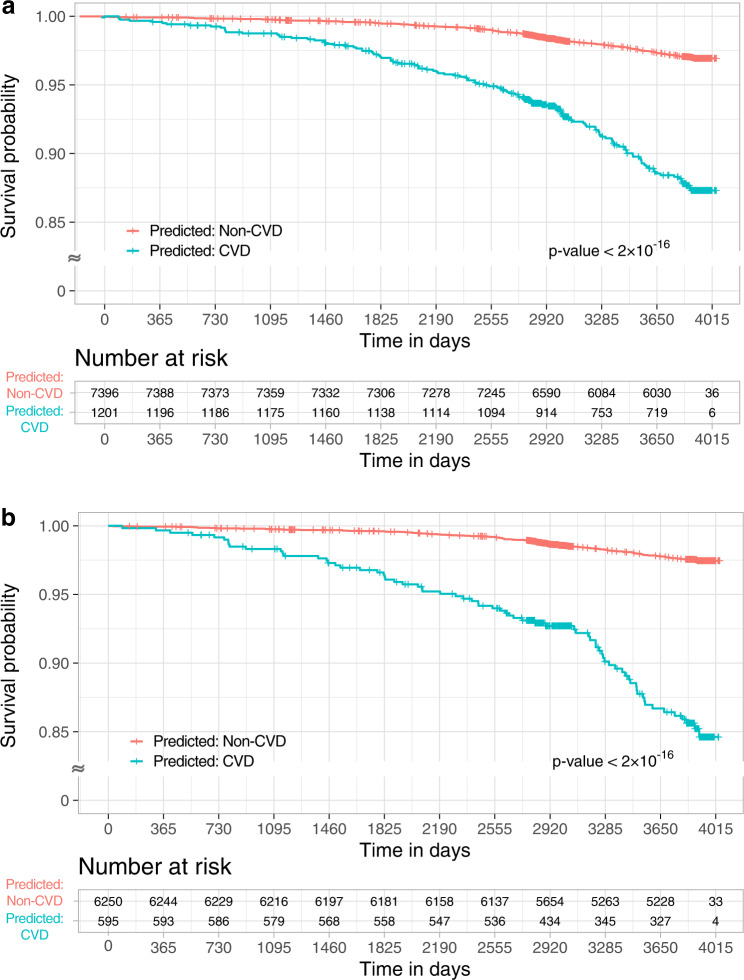
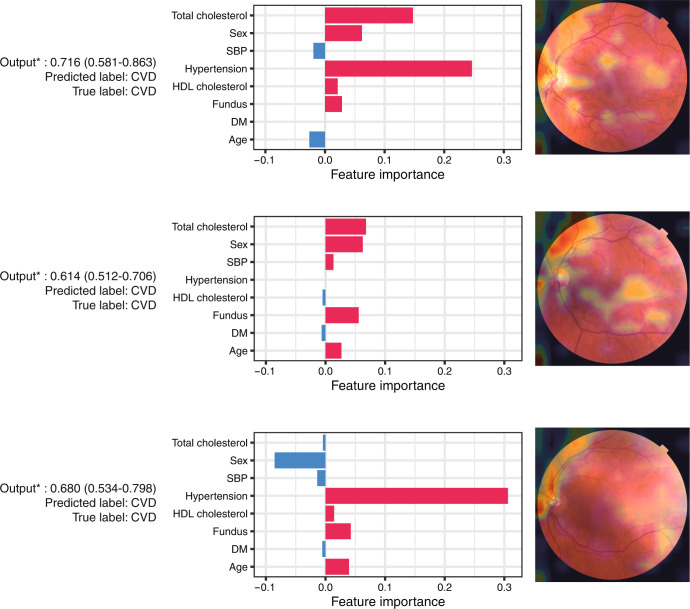
Cardiovascular disease (CVD), the leading cause of death globally, is associated with complicated underlying risk factors. We develop an artificial intelligence model to identify CVD using multimodal data, including clinical risk factors and fundus photographs from the Samsung Medical Center (SMC) for development and internal validation and from the UK Biobank for external validation. The multimodal model achieves an area under the receiver operating characteristic curve (AUROC) of 0.781 (95% confidence interval [CI] 0.766-0.798) in the SMC and 0.872 (95% CI 0.857-0.886) in the UK Biobank. We further observe a significant association between the incidence of CVD and the predicted risk from at-risk patients in the UK Biobank (hazard ratio [HR] 6.28, 95% CI 4.72-8.34). We visualize the importance of individual features in photography and traditional risk factors. The results highlight that non-invasive fundus photography can be a possible predictive marker for CVD.
© 2023. The Author(s).
Conflict of interest statement
Woong-Yang Park was employed by the commercial company GENINUS. The remaining authors declare no competing financial or non-financial interests.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
