Biomechanical and Mechanobiological Drivers of the Transition From PostCapillary Pulmonary Hypertension to Combined Pre-/PostCapillary Pulmonary Hypertension
- PMID: 36734341
- PMCID: PMC9973648
- DOI: 10.1161/JAHA.122.028121
Biomechanical and Mechanobiological Drivers of the Transition From PostCapillary Pulmonary Hypertension to Combined Pre-/PostCapillary Pulmonary Hypertension
Abstract
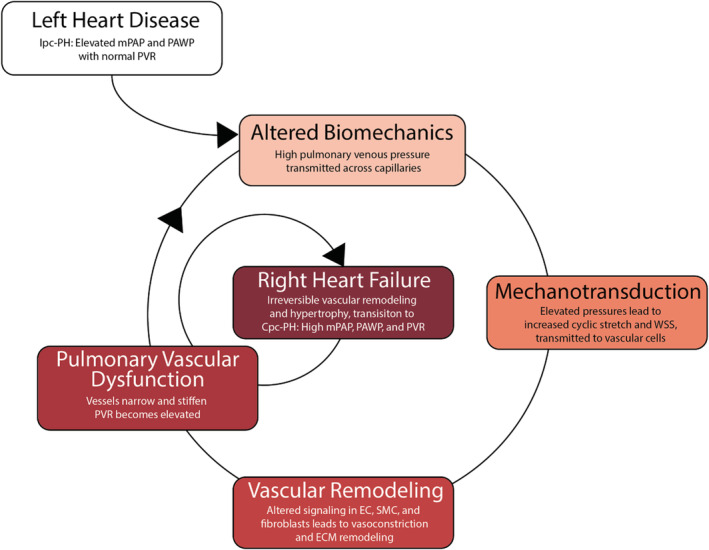
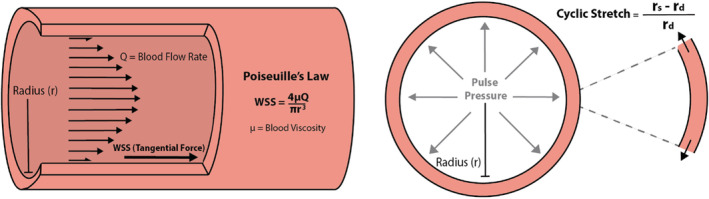
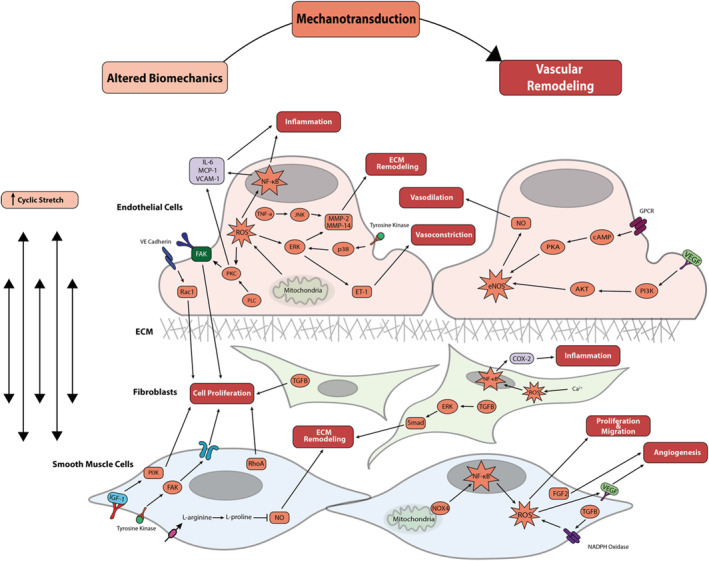
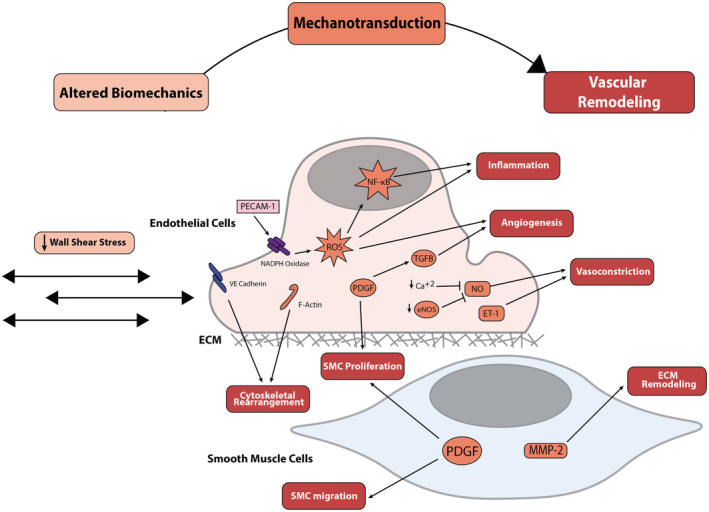
Combined pre-/postcapillary pulmonary hypertension (Cpc-PH), a complication of left heart failure, is associated with higher mortality rates than isolated postcapillary pulmonary hypertension alone. Currently, knowledge gaps persist on the mechanisms responsible for the progression of isolated postcapillary pulmonary hypertension (Ipc-PH) to Cpc-PH. Here, we review the biomechanical and mechanobiological impact of left heart failure on pulmonary circulation, including mechanotransduction of these pathological forces, which lead to altered biological signaling and detrimental remodeling, driving the progression to Cpc-PH. We focus on pathologically increased cyclic stretch and decreased wall shear stress; mechanotransduction by endothelial cells, smooth muscle cells, and pulmonary arterial fibroblasts; and signaling-stimulated remodeling of the pulmonary veins, capillaries, and arteries that propel the transition from Ipc-PH to Cpc-PH. Identifying biomechanical and mechanobiological mechanisms of Cpc-PH progression may highlight potential pharmacologic avenues to prevent right heart failure and subsequent mortality.
Keywords: biomechanics; mechanotransduction; pulmonary hypertension due to left heart failure; pulmonary vascular remodeling.
Figures