

Two-year efficacy and safety of risdiplam in patients with type 2 or non-ambulant type 3 spinal muscular atrophy (SMA)
- PMID: 36735057
- PMCID: PMC9897618
- DOI: 10.1007/s00415-023-11560-1
Two-year efficacy and safety of risdiplam in patients with type 2 or non-ambulant type 3 spinal muscular atrophy (SMA)
Erratum in
-
Correction to: Two‑year efficacy and safety of risdiplam in patients with type 2 or non‑ambulant type 3 spinal muscular atrophy (SMA).J Neurol. 2023 May;270(5):2547-2549. doi: 10.1007/s00415-023-11658-6. J Neurol. 2023. PMID: 37071150 Free PMC article. No abstract available.
Abstract
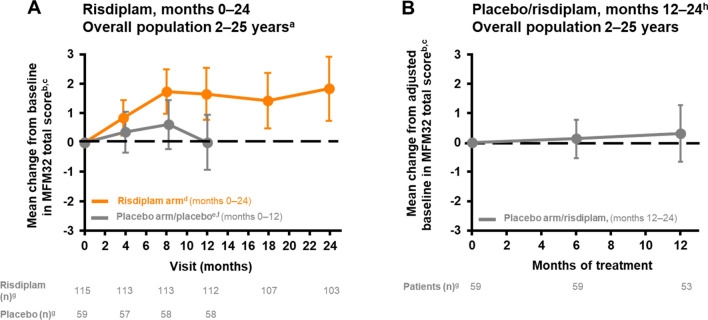
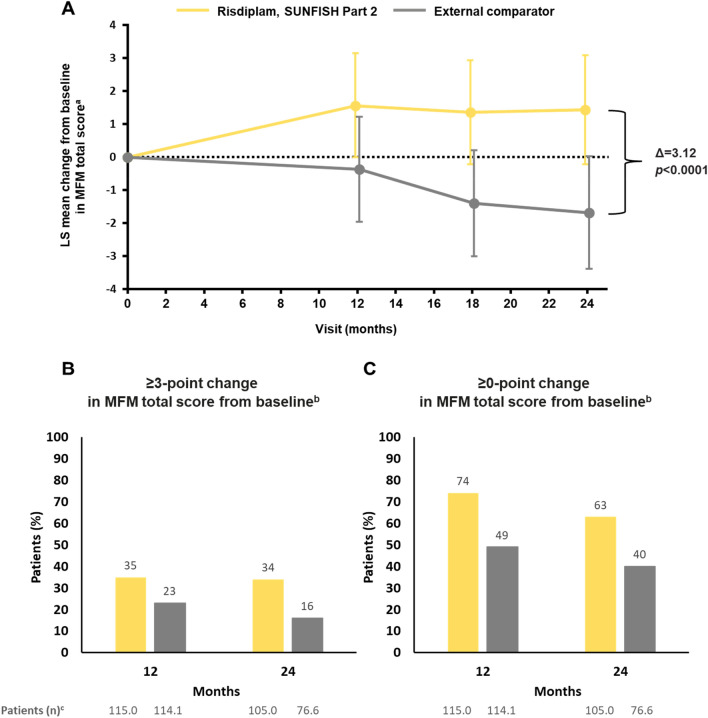
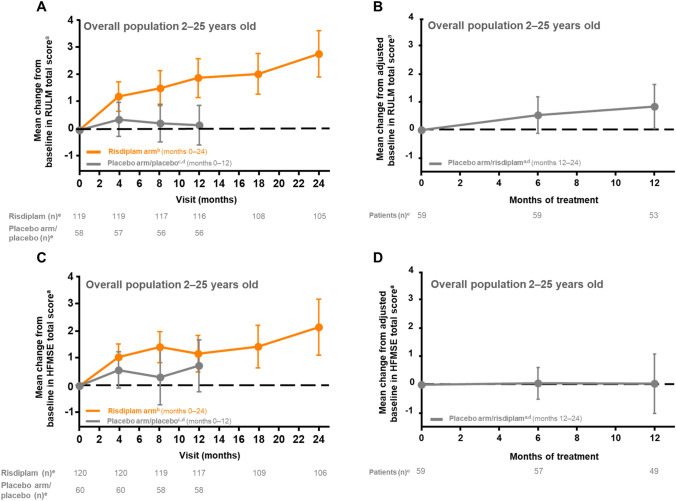
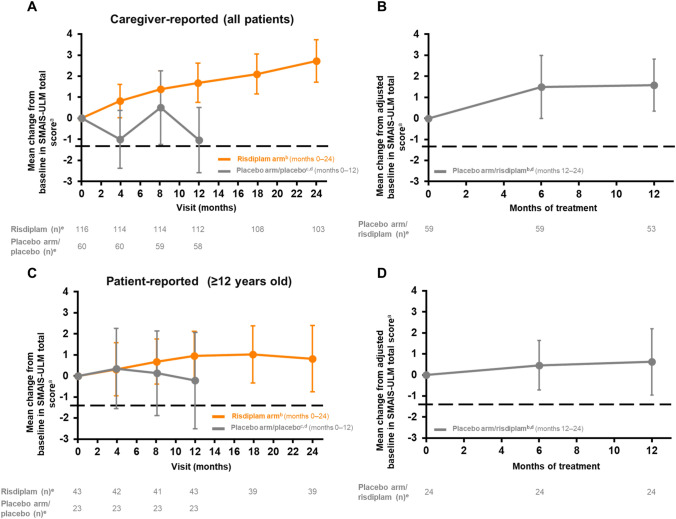
Risdiplam is an oral, survival of motor neuron 2 (SMN2) pre-mRNA splicing modifier approved for the treatment of spinal muscular atrophy (SMA). SUNFISH (NCT02908685) Part 2, a Phase 3, randomized, double-blind, placebo-controlled study, investigated the efficacy and safety of risdiplam in type 2 and non‑ambulant type 3 SMA. The primary endpoint was met: a significantly greater change from baseline in 32-item Motor Function Measure (MFM32) total score was observed with risdiplam compared with placebo at month 12. After 12 months, all participants received risdiplam while preserving initial treatment blinding. We report 24-month efficacy and safety results in this population. Month 24 exploratory endpoints included change from baseline in MFM32 and safety. MFM‑derived results were compared with an external comparator. At month 24 of risdiplam treatment, 32% of patients demonstrated improvement (a change of ≥ 3) from baseline in MFM32 total score; 58% showed stabilization (a change of ≥ 0). Compared with an external comparator, a treatment difference of 3.12 (95% confidence interval [CI] 1.67-4.57) in favor of risdiplam was observed in MFM-derived scores. Overall, gains in motor function at month 12 were maintained or improved upon at month 24. In patients initially receiving placebo, MFM32 remained stable compared with baseline (0.31 [95% CI - 0.65 to 1.28]) after 12 months of risdiplam; 16% of patients improved their score and 59% exhibited stabilization. The safety profile after 24 months was consistent with that observed after 12 months. Risdiplam over 24 months resulted in further improvement or stabilization in motor function, confirming the benefit of longer-term treatment.
Keywords: Motor function; Risdiplam; SMA; SUNFISH; Safety; Spinal muscular atrophy.
© 2023. The Author(s).
Conflict of interest statement
MO reports grants from F. Hoffmann-La Roche Ltd during the conduct of the study and has received grants as a clinical trial investigator from Biogen. JWD has received fees for serving on scientific advisory boards from Biogen, Novartis, Sarepta Therapeutics, and Avidity; has received consulting fees from Affinia Therapeutics and Shift Therapeutics for a therapeutic platform; and has received grant support for clinical trials from F. Hoffmann-La Roche Ltd, Biogen, Novartis Gene Therapies, Cytokinetics, Scholar Rock, and Sarepta Therapeutics. ND served on scientific advisory boards for F. Hoffmann-La Roche Ltd, Biogen and Novartis Pharmaceuticals; he has received personal fees from Biogen and F. Hoffmann-La Roche Ltd for congress and travel support. ESM reports that she has served on advisory boards for Biogen and Scholar Rock. She has received consulting fees, travel support, and speaker honoraria as an independent contractor from F. Hoffmann-La Roche Ltd, Biogen, AveXis, and Scholar Rock. AN has received fees for serving on scientific advisory boards and speaker fees from F. Hoffmann-La Roche Ltd. KS reports grants from F. Hoffmann-La Roche Ltd/Chugai Pharmaceutical during the conduct of the study and grants from Biogen Japan and lecture fees from Novartis Pharmaceuticals, outside the submitted work. CV reports personal fees and financial support to her institution from F. Hoffmann-La Roche Ltd for activities outside the submitted work. GB received consultancy fees and speaker honoraria from F. Hoffmann-La Roche Ltd, AveXis/Novartis Gene Therapy, and Biogen, and grants from F. Hoffmann-La Roche Ltd. NG reports fees for serving on advisory boards and presentations at symposia from F. Hoffmann-La Roche Ltd, Biogen, AveXis, and Novartis. JK received grants or contracts from Novartis Gene Therapies and Biogen. He has received consulting and speaker fees from F. Hoffmann La Roche Ltd, Biogen, and Novartis Gene Therapies and consulting fees from Scholar Rock. AK-P reports that she received an institutional support grant from Biogen; serving on scientific advisory boards for and receiving speaker honoraria from Biogen, F. Hoffmann-La Roche Ltd, Novartis, and PTC Therapeutics; and receiving personal fees from Biogen and F. Hoffmann-La Roche Ltd for travel support. LS received grants and personal fees from F. Hoffmann-La Roche Ltd, Biogen, and AveXis/Novartis Gene Therapies and personal fees from Cytokinetics, BioHaven, and Scholar Rock, outside the submitted work. GP, KG, HK, CM, TM, RSS, HS, WYY, and PF report that they are current employees of and stockholders in F. Hoffmann-La Roche Ltd. EM has received fees for serving on scientific advisory boards; speaker fees from F. Hoffmann-La Roche Ltd, Biogen, AveXis/Novartis, Scholar Rock, and Cytokinetics; and grants from Biogen during the conduct of the study.
Figures
References
-
- Mercuri E, Darras BT, Chiriboga CA, Day JW, Campbell C, Connolly AM, Iannaccone ST, Kirschner J, Kuntz NL, Saito K, Shieh PB, Tulinius M, Mazzone ES, Montes J, Bishop KM, Yang Q, Foster R, Gheuens S, Bennett CF, Farwell W, Schneider E, De Vivo DC, Finkel RS, Group CS Nusinersen versus sham control in later-onset spinal muscular atrophy. The N Engl J Med. 2018;378:625–635. doi: 10.1056/NEJMoa1710504. - DOI - PubMed
-
- Mercuri E, Lucibello S, Pera MC, Carnicella S, Coratti G, de Sanctis R, Messina S, Mazzone E, Forcina N, Fanelli L, Norcia G, Antonaci L, Frongia AL, Pane M. Long-term progression in type II spinal muscular atrophy: a retrospective observational study. Neurology. 2019;93:e1241–e1247. doi: 10.1212/WNL.0000000000008166. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
