

Dose-Response Relationship between Obstructive Sleep Apnea Therapy Adherence and Healthcare Utilization
- PMID: 36735928
- PMCID: PMC10257023
- DOI: 10.1513/AnnalsATS.202208-738OC
Dose-Response Relationship between Obstructive Sleep Apnea Therapy Adherence and Healthcare Utilization
Abstract
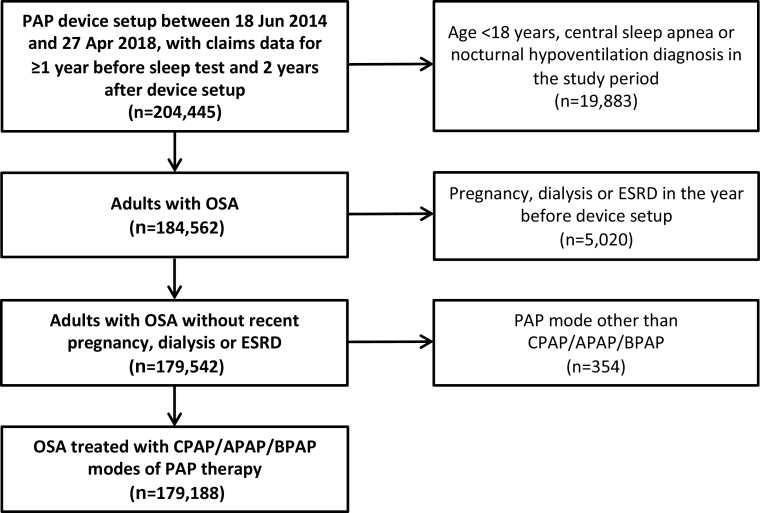
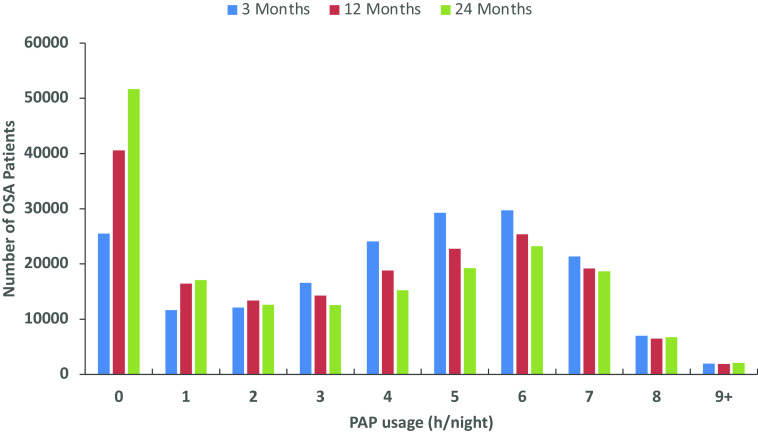
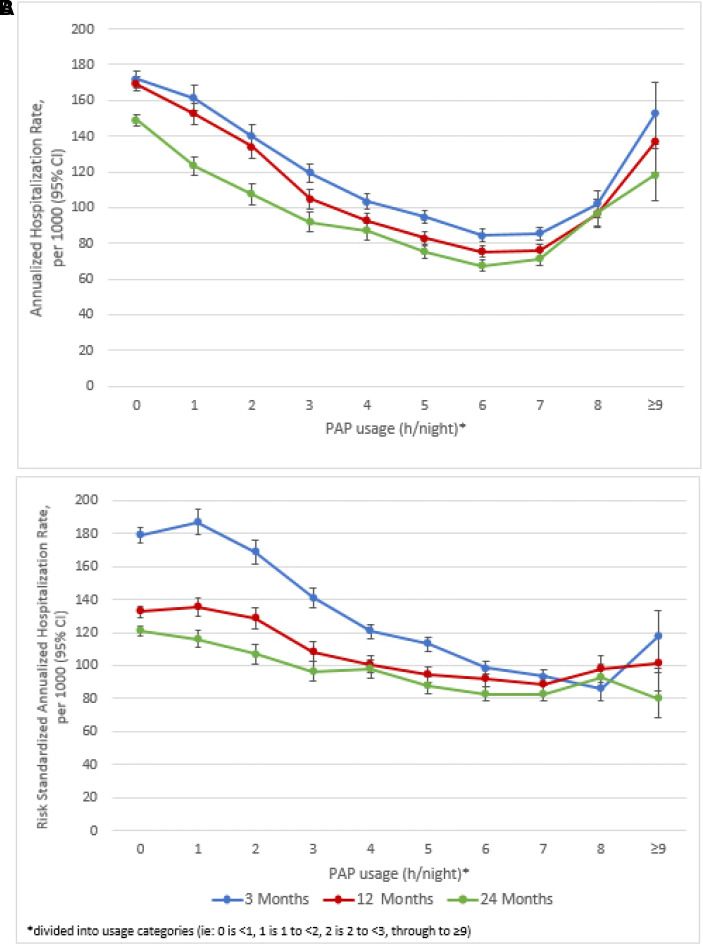
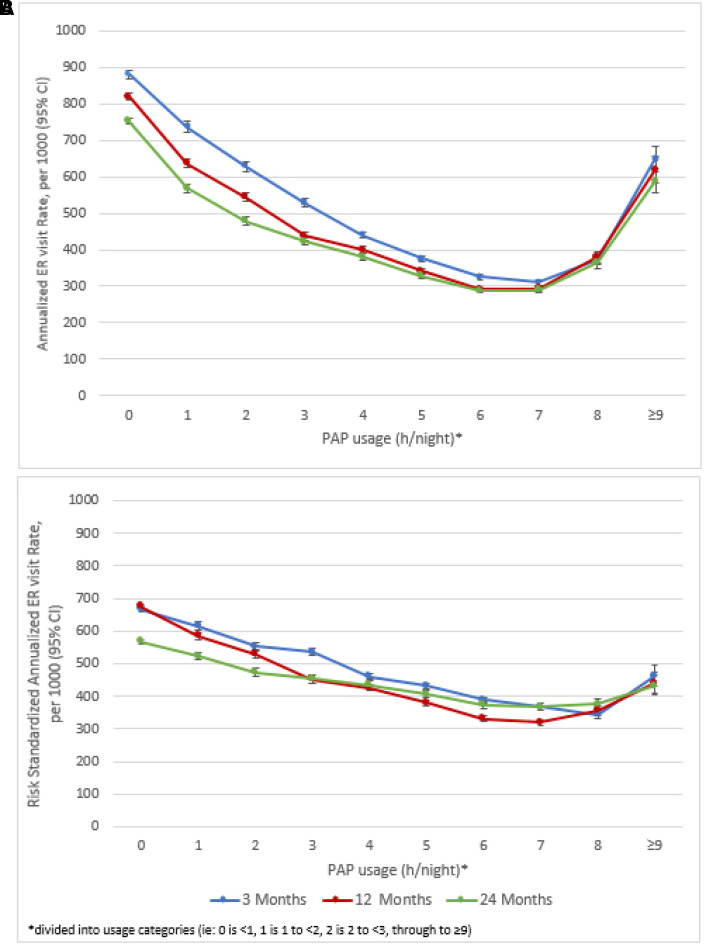
Rationale: Clear definition of optimal positive airway pressure therapy usage in patients with obstructive sleep apnea is not possible because of scarce data on the relationship between usage hours and major clinical outcomes. Objective: To investigate the dose-response relationship between positive airway pressure usage and healthcare resource utilization and determine the minimum device usage required for benefit. Methods: A linked data set combined deidentified payer-sourced administrative medical/pharmacy claims data from more than 100 U.S. health plans and individual patient positive airway pressure usage data. Eligible adults (age ⩾18 yr) had a new obstructive sleep apnea diagnosis between June 2014 and April 2018. All received positive airway pressure therapy (AirSense 10; ResMed) with claims data for ⩾1 year before, and 2 years after, device setup. Healthcare resource utilization was determined on the basis of the number of all-cause hospitalizations and emergency room visits over 3, 12, and 24 months after positive airway pressure initiation. Results: Data from 179,188 patients showed a clear dose-response relationship between daily positive airway pressure usage and healthcare utilization. Minimum device usage required for benefit was 1-3 hours per night. There was a statistically significant decrease in hospitalizations and emergency room visits at all time points (all Ps < 0.0001) with increasing positive airway pressure usage. Each additional hour of usage per night decreased hospitalizations and emergency room visits by 5-10% and 5-7%, respectively. Conclusions: These data provide compelling evidence for a dose-response relationship between positive airway pressure usage and healthcare utilization, with benefits seen even when usage was as low as 1-2 hours per night.
Keywords: OSA; dose–response; emergency room visits; healthcare resource utilization; hospitalization; positive airway pressure.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
