

High central venous pressure amplitude predicts successful defibrillation in a porcine model of cardiac arrest
- PMID: 36736947
- PMCID: PMC11087940
- DOI: 10.1016/j.resuscitation.2023.109716
High central venous pressure amplitude predicts successful defibrillation in a porcine model of cardiac arrest
Abstract
Aim: Increasing venous return during cardiopulmonary resuscitation (CPR) has been shown to improve hemodynamics during CPR and outcomes following cardiac arrest (CA). We hypothesized that a high central venous pressure amplitude (CVP-A), the difference between the maximum and minimum central venous pressure during chest compressions, could serve as a robust predictor of return of spontaneous circulation (ROSC) in addition to traditional measurements of coronary perfusion pressure (CPP) and end-tidal CO2 (etCO2) in a porcine model of CA.
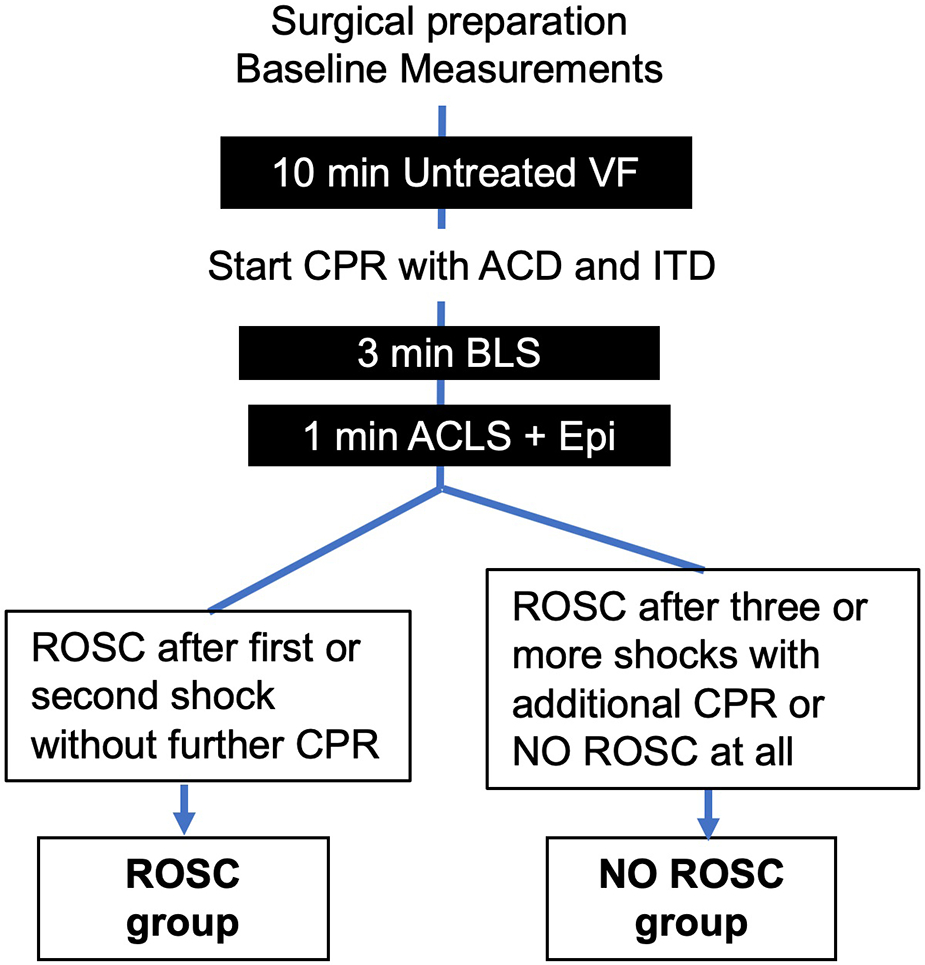
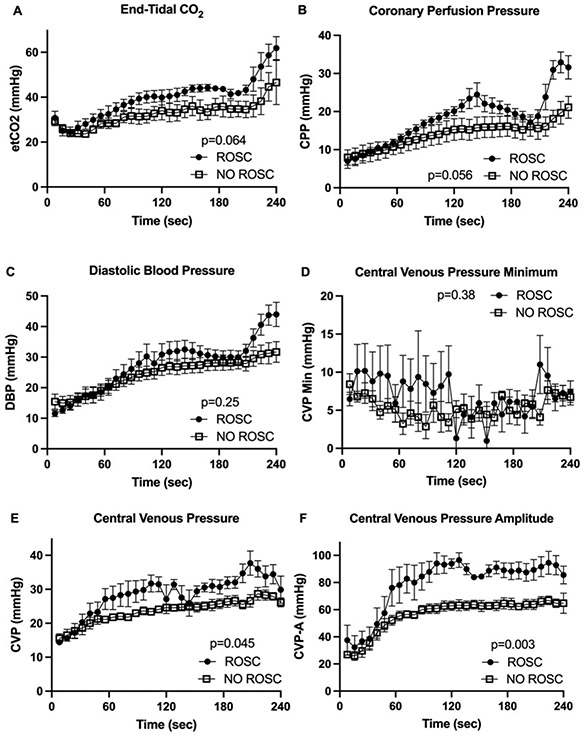
Methods: After 10 min of ventricular fibrillation, 9 anesthetized and intubated female pigs received mechanical chest compressions with active compression/decompression (ACD) and an impedance threshold device (ITD). CPP, CVP-A and etCO2 were measured continuously. All groups received biphasic defibrillation (200 J) at minute 4 of CPR and were classified into two groups (ROSC, NO ROSC). Mean values were analyzed over 3 min before defibrillation by repeated-measures Analysis of Variance and receiver operating characteristic (ROC).
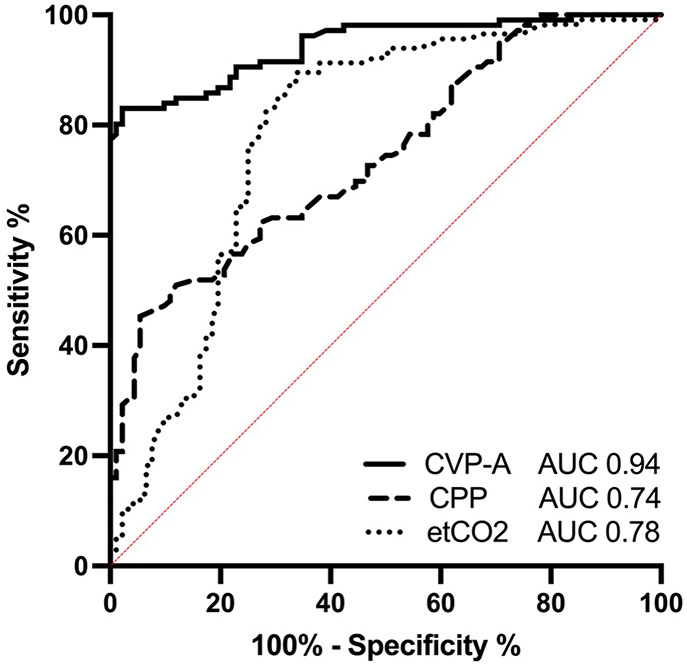
Results: Five animals out of 9 experienced ROSC. CVP-A showed a statistically significant difference (p = 0.003) between the two groups during 3 min of CPR before defibrillation compared to CPP (p = 0.056) and etCO2 (p = 0.064). Areas-under-the-curve in ROC analysis for CVP-A, CPP and etCO2 were 0.94 (95% Confidence Interval 0.86, 1.00), 0.74 (0.54, 0.95) and 0.78 (0.50, 1.00), respectively.
Conclusion: In our study, CVP-A was a potentially useful predictor of successful defibrillation and return of spontaneous circulation. Overall, CVP-A could serve as a marker for prediction of ROSC with increased venous return and thereby monitoring the beneficial effects of ACD and ITD.
Keywords: Cardiopulmonary resuscitation; Central venous pressure; Coronary perfusion pressure; End-tidal CO2; Return of spontaneous circulation; Ventricular fibrillation.
Published by Elsevier B.V.
Conflict of interest statement
Conflicts of interest
None
Figures
Comment in
-
Central venous pressure amplitude: A novel marker of resuscitation quality.Resuscitation. 2023 Apr;185:109749. doi: 10.1016/j.resuscitation.2023.109749. Epub 2023 Feb 25. Resuscitation. 2023. PMID: 36842673 No abstract available.
References
-
- Gräsner J-T, Lefering R, Koster RW, et al. EuReCa ONE—27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016;105:188–195. - PubMed
-
- Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141(9):e139–e596. - PubMed
-
- Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S366–S468. - PubMed
-
- Lurie KG, Lindo C, Chin J. CPR: the P stands for plumber’s helper. JAMA. 1990;264(13):1661. - PubMed
-
- Lurie KG, Coffeen P, Shultz J, McKnite S, Detloff B, Mulligan K. Improving active compression-decompression cardiopulmonary resuscitation with an inspiratory impedance valve. Circulation. 1995;91(6):1629–1632. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
