

Trends and Variation in Pediatric Anaphylaxis Care From 2016 to 2022
- PMID: 36736955
- PMCID: PMC10085823
- DOI: 10.1016/j.jaip.2023.01.029
Trends and Variation in Pediatric Anaphylaxis Care From 2016 to 2022
Abstract
Background: Variation in the use of treatments and hospitalization for anaphylaxis would suggest a lack of consensus in therapeutic approach.
Objective: To evaluate trends and practice variation in the emergency department (ED) care of children with anaphylaxis in a large US cohort.
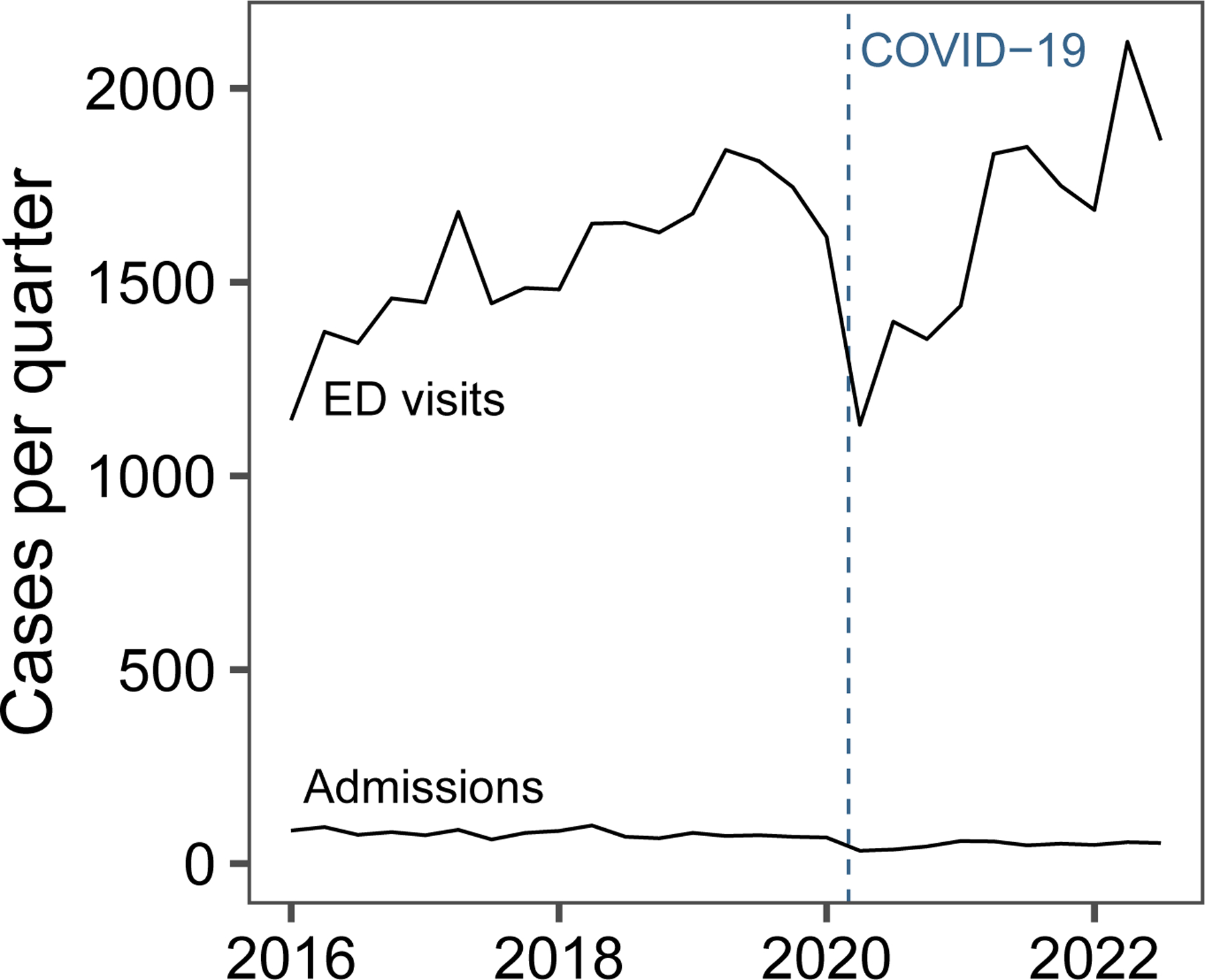
Methods: We conducted a 48-site retrospective cohort study using the Pediatric Health Information System from January 2016 through September 2022. Children younger than 18 years with a primary diagnosis of anaphylaxis were included. Care trends were assessed using negative binomial regression modeling. Rates of medication use, hospitalizations, and revisits were reported as medians with interquartile ranges (IQRs).
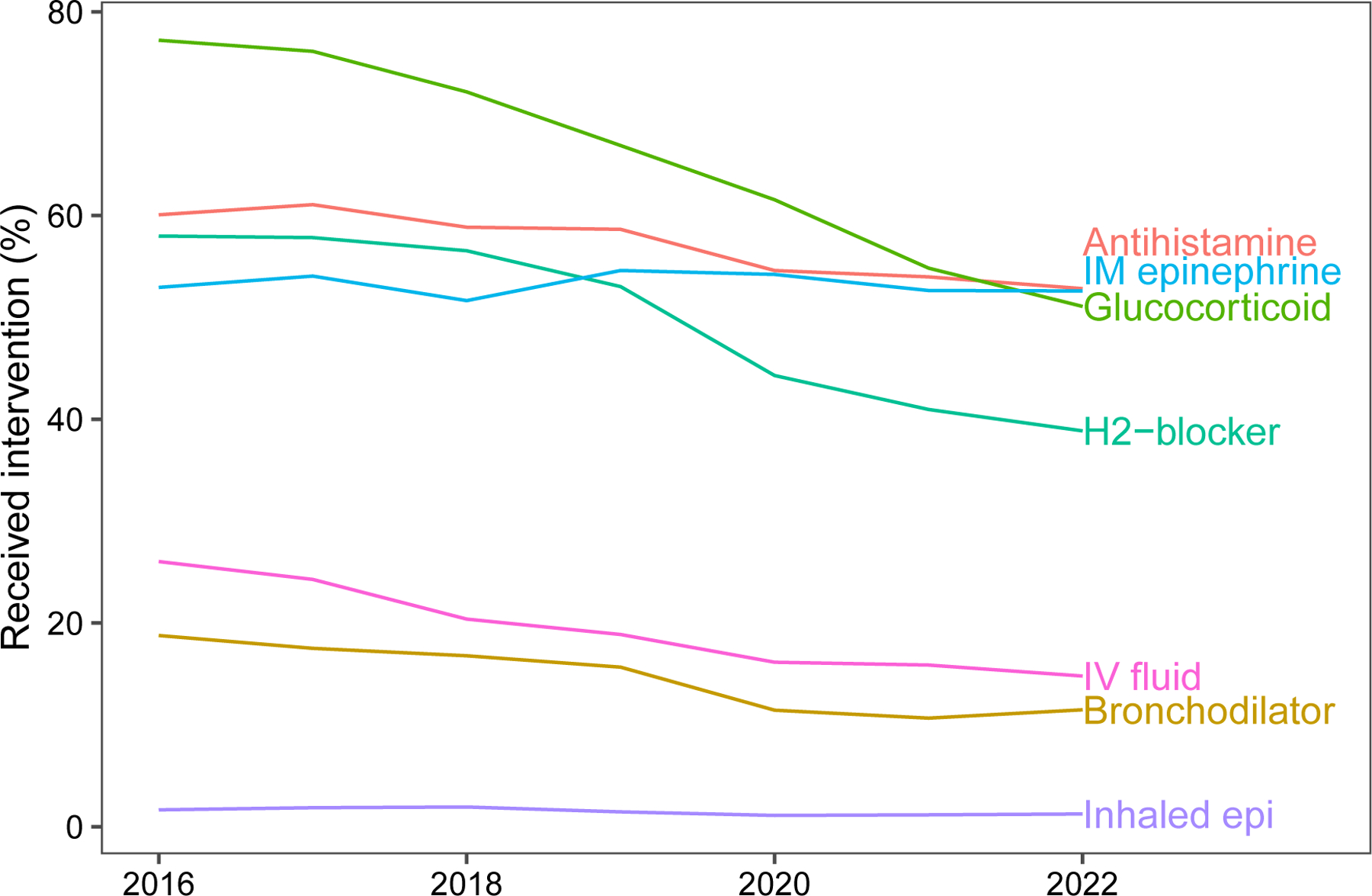
Results: There were 42,909 ED visits for anaphylaxis, with a 4.2% per-year increase in visit incidence (95% CI, 1.8-6.7) during the study period. The median hospitalization rate was 3.5% (IQR, 2.2-6.0), and the 3-day ED revisit rate was 0.6% (IQR, 0.4-0.9). The hospital-level median use of therapies included intramuscular epinephrine (55.3%; IQR, 50.1-59.9), systemic steroids (73.8%; IQR, 63.9-81.4), antihistamines (59.9%; IQR, 53.5-65.5), H2-receptor antagonists (56.8%; IQR, 42.3-66.2), bronchodilators (15.1%; IQR, 12.5-17.0), inhaled epinephrine (1.1%; IQR, 0.6-1.9), and fluid boluses (19.8%; IQR, 11.3-29.3). Severe reactions requiring intensive care unit admission (1.5%; IQR, 0.8-2.2), vasopressors (0.3%; IQR, 0.0-0.6), and intubation (0.2%; IQR, 0.0-0.3) were rare.
Conclusions: ED visits for anaphylaxis increased during the study period, but hospitalization rates were low. Substantial variation exists between EDs regarding the use of anaphylaxis therapies, supporting the need for future research to evaluate the efficacy of these medications.
Keywords: Anaphylaxis; Antihistamines; Bronchodilators; Corticosteroids; Emergency department; Epinephrine; Hospitalizations; Trends; Variation.
Copyright © 2023 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117(2):391–7. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0091674905027235 - PubMed
-
- Turner PJ, Campbell DE, Motosue MS, Campbell RL. Global Trends in Anaphylaxis Epidemiology and Clinical Implications. J Allergy Clin Immunol Pract. 2020;8(4):1169–76. Available from: https://www.sciencedirect.com/science/article/pii/S2213219819309675 - PMC - PubMed
-
- Michelson KA, Dribin TE, Vyles D, Neuman MI. Trends in emergency care for anaphylaxis. J Allergy Clin Immunol Pract. 2020;8(2):767–768.e2. - PubMed
-
- Dribin TE, Michelson KA, Monuteaux MC, Schnadower D, Neuman MI. Timing and predictors of repeat epinephrine administration among children hospitalized for anaphylaxis. J Allergy Clin Immunol Pract. 2020;8:1400–1402.e2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
