

Letter to the Editor: clinical utility of urine DNA for noninvasive detection and minimal residual disease monitoring in urothelial carcinoma
- PMID: 36739413
- PMCID: PMC9898696
- DOI: 10.1186/s12943-023-01729-7
Letter to the Editor: clinical utility of urine DNA for noninvasive detection and minimal residual disease monitoring in urothelial carcinoma
Abstract
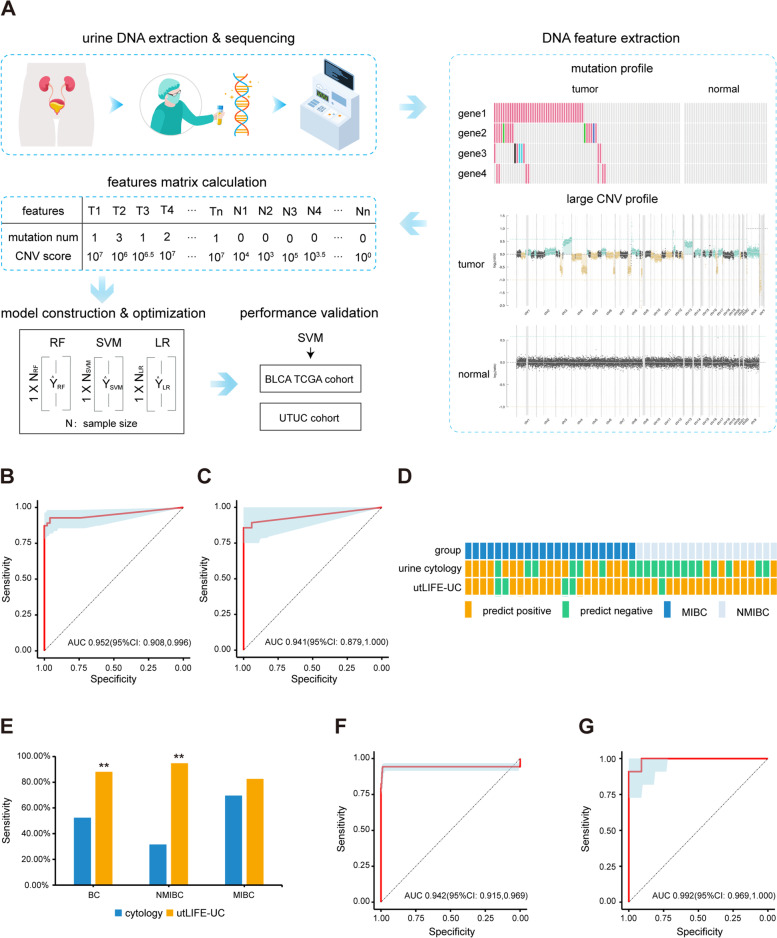
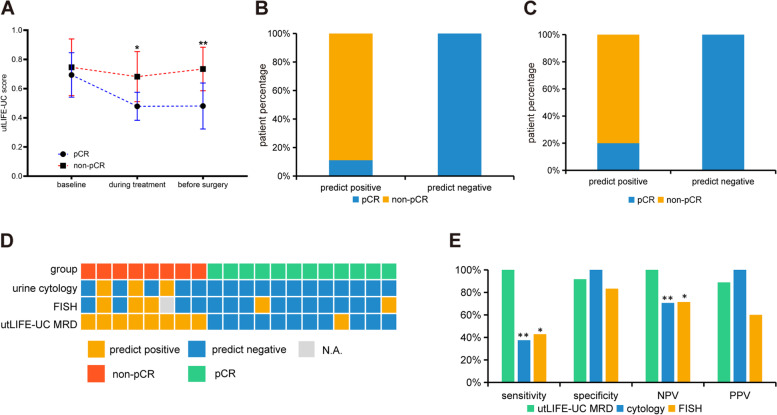
Current methods for the early detection and minimal residual disease (MRD) monitoring of urothelial carcinoma (UC) are invasive and/or possess suboptimal sensitivity. We developed an efficient workflow named urine tumor DNA multidimensional bioinformatic predictor (utLIFE). Using UC-specific mutations and large copy number variations, the utLIFE-UC model was developed on a bladder cancer cohort (n = 150) and validated in The Cancer Genome Atlas (TCGA) bladder cancer cohort (n = 674) and an upper tract urothelial carcinoma (UTUC) cohort (n = 22). The utLIFE-UC model could discriminate 92.8% of UCs with 96.0% specificity and was robustly validated in the BLCA_TCGA and UTUC cohorts. Furthermore, compared to cytology, utLIFE-UC improved the sensitivity of bladder cancer detection (p < 0.01). In the MRD cohort, utLIFE-UC could distinguish 100% of patients with residual disease, showing superior sensitivity compared to cytology (p < 0.01) and fluorescence in situ hybridization (FISH, p < 0.05). This study shows that utLIFE-UC can be used to detect UC with high sensitivity and specificity in patients with early-stage cancer or MRD. The utLIFE-UC is a cost-effective, rapid, high-throughput, noninvasive, and promising approach that may reduce the burden of cystoscopy and blind surgery.
Keywords: Early detection; MRD; Urine DNA; Urothelial carcinoma; utLIFE.
© 2023. The Author(s).
Conflict of interest statement
H-N Wang, Z-X Guo, F Ding, T Zhou, W Wang, Y-K Wang, L Liu, J Guo, S-P Zhu, X-H Zhang, S-B Cao, and F Lou are employed by Acornmed Biotechnology Co., Ltd. The other authors declare no conflicts of interest.
Figures
References
-
- Cumberbatch MGK, Jubber I, Black PC, Esperto F, Figueroa JD, Kamat AM, Kiemeney L, Lotan Y, Pang K, Silverman DT, et al. Epidemiology of bladder Cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018;74(6):784–795. doi: 10.1016/j.eururo.2018.09.001. - DOI - PubMed
-
- Matsumoto K, Novara G, Gupta A, Margulis V, Walton TJ, Roscigno M, Ng C, Kikuchi E, Zigeuner R, Kassouf W, et al. Racial differences in the outcome of patients with urothelial carcinoma of the upper urinary tract: an international study. BJU Int. 2011;108(8 Pt 2):E304–E309. doi: 10.1111/j.1464-410X.2011.10188.x. - DOI - PubMed
-
- Rouprêt M, Babjuk M, Burger M, Capoun O, Cohen D, Compérat EM, Cowan NC, Dominguez-Escrig JL, Gontero P, Hugh Mostafid A, et al. European Association of Urology guidelines on upper urinary tract Urothelial carcinoma: 2020 update. Eur Urol. 2021;79(1):62–79. doi: 10.1016/j.eururo.2020.05.042. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
