

Hard and soft tissue regeneration of severe peri-implantitis defects with the laser-assisted peri-implant defect regeneration technique: 3-year results
- PMID: 36739596
- PMCID: PMC9899875
- DOI: 10.1186/s40729-023-00467-1
Hard and soft tissue regeneration of severe peri-implantitis defects with the laser-assisted peri-implant defect regeneration technique: 3-year results
Abstract
Purpose: This retrospective cohort study evaluates the regeneration of severe peri-implantitis deficiencies treated with the laser-assisted peri-implant defect regeneration (LAPIDER) approach within a 3-year follow-up.
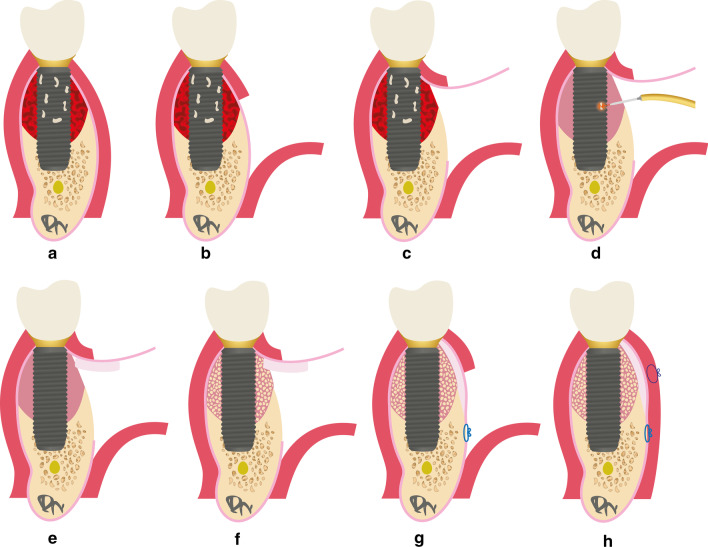
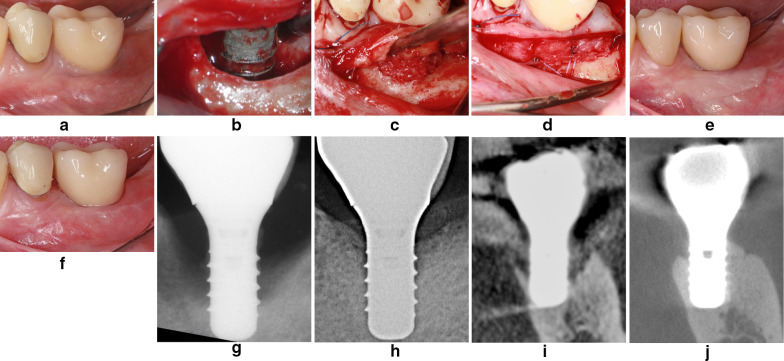
Methods: Twenty-four implants with severe peri-implantitis in 18 patients were treated according to the LAPIDER technique. In contrast to classic techniques for reconstructive peri-implantitis surgery with a marginal incision, a buccal split-flap preparation avoiding papillae separation was used. After a coronal flap elevation and a laser-assisted peri-implant defect cleaning, connective tissue and autogenous bone grafting was performed. Primary outcomes were the changes of the marginal bone levels (MBL) and the buccal bone thickness. Secondary outcomes included implant survival, peri-implant probing depths (PPD), bleeding on probing (BOP), recession, width of keratinized mucosa (KMW), thickness of keratinized mucosa (KMT), soft tissue esthetics (PES), and implant success.
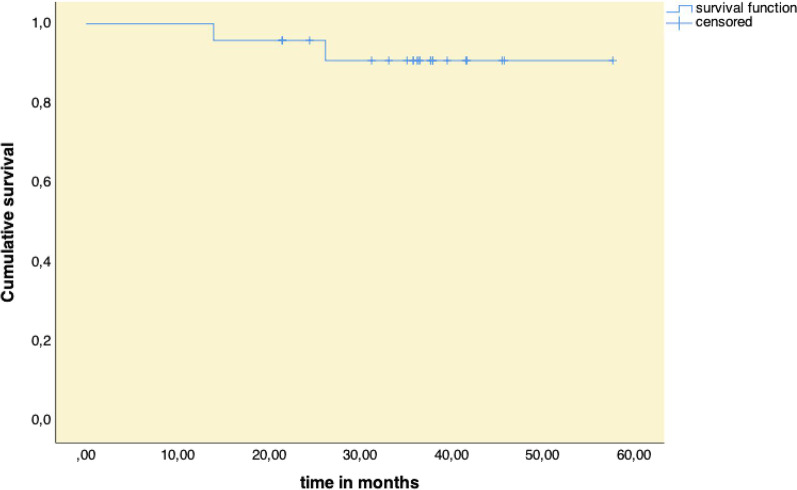
Results: MBL improved interproximal by 3.10 ± 2.02 mm (p < 0.001), buccal by 3.49 ± 2.89 mm (p < 0.001), and lingual by 1.46 ± 1.98 mm (p = 0.003); buccal bone thickness by 0.55 ± 0.60 mm (p = 0.005), and 1.01 ± 1.25 mm (p = 0.001) at 1 and 3 mm below reference level. Two implants were removed; 22 implants were still in function at a mean follow-up of 36 months. PPD changed from 5.05 ± 1.39 to 3.08 ± 0.71 mm (p < 0.001); recession was reduced from 2.07 ± 1.70 to 0.91 ± 1.13 mm (p = 0.001); KMW increased from 2.91 ± 1.81 to 4.18 ± 1.67 mm (p = 0.006); KMT improved from 1.73 ± 0.50 to 2.44 ± 0.43 mm (p < 0.001); PES changed from 7.7 ± 2.8 to 10.7 ± 1.9 (p < 0.001). 45.8% to 54.2% of the implants met the criteria of implant success.
Conclusions: The favorable results document the proof of principle for the regeneration of severe peri-implant hard and soft tissue deficiencies by the LAPIDER treatment approach.
Keywords: Bone graft; Bone regeneration; Dental implant; Keratinized mucosa; Peri-implantitis; Recession; Reconstructive therapy; Soft tissue graft; Surface decontamination.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Carcuac O, Derks J, Abrahamsson I, Wennstrom JL, Petzold M, Berglundh T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J Clin Periodontol. 2017;44(12):1294–1303. - PubMed
-
- Schwarz F, John G, Schmucker A, Sahm N, Becker J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: a 7-year follow-up observation. J Clin Periodontol. 2017;44(3):337–342. - PubMed
-
- Tomasi C, Regidor E, Ortiz-Vigon A, Derks J. Efficacy of reconstructive surgical therapy at peri-implantitis-related bone defects. a systematic review and meta-analysis. J Clin Periodontol. 2019;46(Suppl 21):340–356. - PubMed
-
- Derks J, Ortiz-Vigon A, Guerrero A, Donati M, Bressan E, Ghensi P, Schaller D, Tomasi C, Karlsson K, Abrahamsson I, Ichioka Y, Dionigi C, Regidor E, Berglundh T. Reconstructive surgical therapy of peri-implantitis: a multicenter randomized controlled clinical trial. Clin Oral Implants Res. 2022;33:921–944. - PMC - PubMed
-
- Renvert S, Giovannoli JL, Roos-Jansaker AM, Rinke S. Surgical treatment of peri-implantitis with or without a deproteinized bovine bone mineral and a native bilayer collagen membrane: a randomized clinical trial. J Clin Periodontol. 2021;48(10):1312–1321. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
