

Mitral Valve Replacement for Enlarged Libman-Sacks Endocarditis in a Patient with Persistent Primary Antiphospholipid Syndrome and Recurrent Stroke: A Case Report
- PMID: 36740820
- PMCID: PMC9909611
- DOI: 10.12659/AJCR.938930
Mitral Valve Replacement for Enlarged Libman-Sacks Endocarditis in a Patient with Persistent Primary Antiphospholipid Syndrome and Recurrent Stroke: A Case Report
Abstract
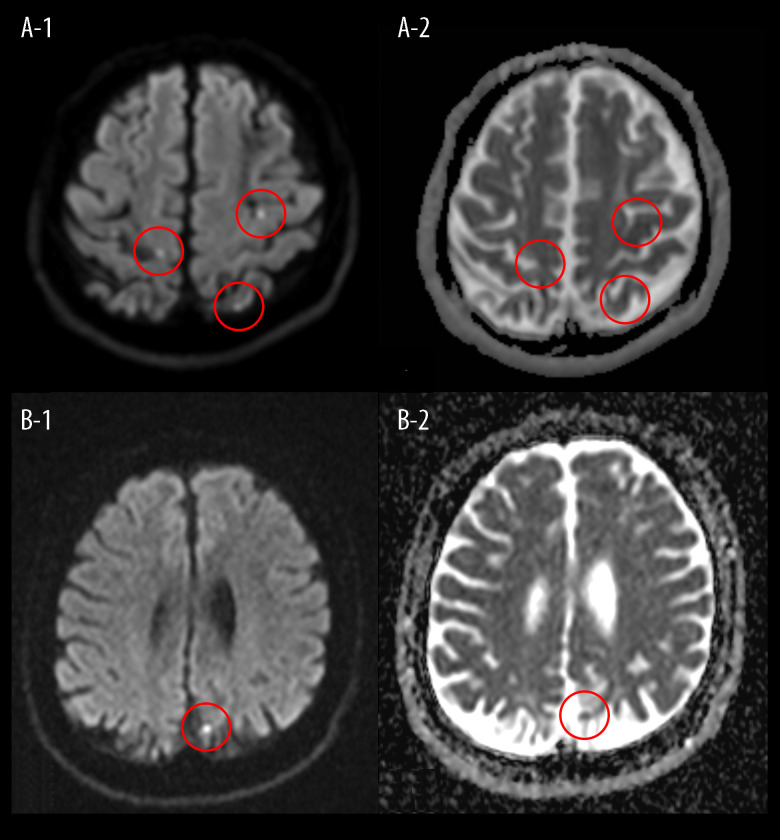
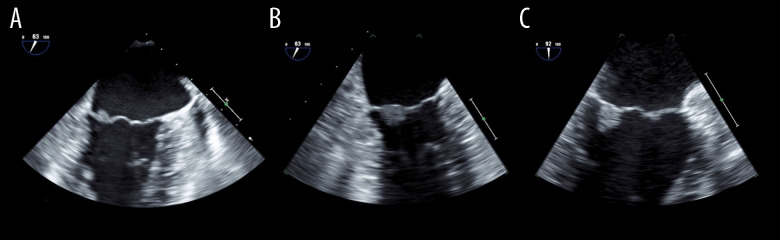
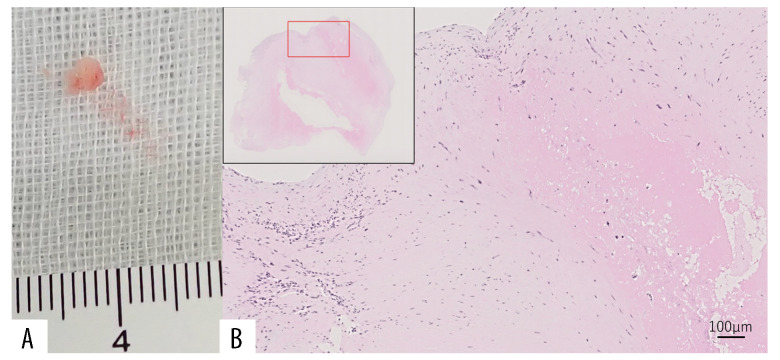
BACKGROUND Anticardiolipin antibodies in patients with Libman-Sacks endocarditis (LS) are indicative of comorbid antiphospholipid syndrome (APS) and can result in cerebral infarctions. We describe a case of LS and primary APS with recurrent cerebral infarctions despite anticoagulation treatment. The patient underwent surgery for enlarged LS vegetation with high titers of antiphospholipid antibodies. CASE REPORT A 41-year-old Japanese man was admitted to hospital for small cerebral infarction recurrence in a left parietal lesion. At age 35, the patient had suffered multiple cerebral infarctions. He was found to have high serum titers of all 3 antiphospholipid antibodies. Transesophageal echocardiography (TEE) findings were normal. Differential diagnosis ruled out other autoimmune diseases and a clinical diagnosis of primary APS was made. Warfarin anticoagulation was started. When cerebral infarction recurred 6 years after the first episode, serum titers of antiphospholipid antibodies remained high, and TEE showed a 7×8 mm area of mitral vegetation. A TEE results from his first admission revealed a 5×6 mm area of mitral vegetation, which was believed to be related to the current vegetation. As anticoagulation produced no improvement, the mitral valve was replaced with a mechanical valve. Examination of the excised vegetation found it to be consistent with LS. The patient made good progress within 3 years after surgery. CONCLUSIONS LS size can increase despite anticoagulation in cases with high titers of all 3 antiphospholipid antibodies and cerebral infarction. Such patients require ongoing TEE follow-up and surgical treatment should be considered.
Conflict of interest statement
Figures
References
-
- Moyssakis I, Tektonidou MG, Vasilliou VA, et al. Libman-Sacks endocarditis in systemic lupus erythematosus: Prevalence, associations, and evolution. Am J Med. 2007;120:636–42. - PubMed
-
- Turiel M, Sarzi-Puttini P, Peretti R, et al. Five-year follow-up by transesophageal echocardiographic studies in primary antiphospholipid syndrome. Am J Cardiol. 2005;96:574–79. - PubMed
-
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost. 2006;4:295–306. - PubMed
-
- Nesher G, Ilany J, Rosenmann D, Abraham AS. Valvular dysfunction in antiphospholipid syndrome: Prevalence, clinical features, and treatment. Semin Arthritis Rheum. 1997;27:27–35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
