

Resistance to single-agent chemotherapy in low-risk gestational trophoblastic neoplasia
- PMID: 36741497
- PMCID: PMC9878912
- DOI: 10.22088/cjim.14.1.47
Resistance to single-agent chemotherapy in low-risk gestational trophoblastic neoplasia
Abstract
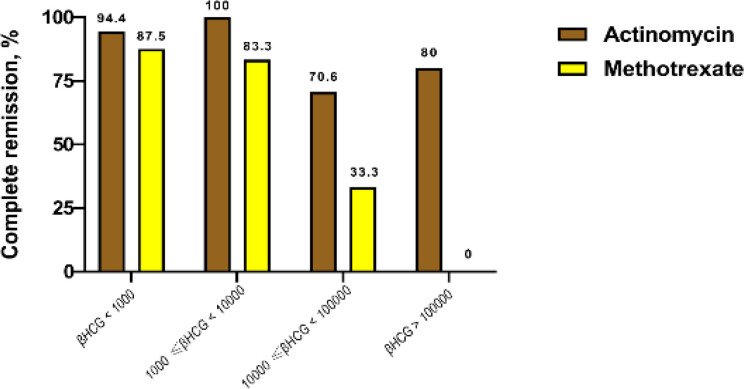
Background: Methotrexate (MTX) and actinomycin D (ActD) have been used as first-line chemotherapy agents in the treatment of low-risk gestational trophoblastic neoplasia (GTN). Although low-risk GTN is considered a curable disease, its reported primary remission rates of 49 to 93% reflect the difficulties of treatment and different factors influencing it. Hence, this study aimed to determine the remission rates and related factors of single-agent chemotherapy resistance in low-risk GTN patients.
Methods: This retrospective study included patients with diagnosed low-risk GTN who received either MTX once a week (IM, 30mg/m2) or ActD once every two weeks (pulsed IV, 1.25mg/m2). Then, the patients were followed-up until complete remission or single-agent treatment failure to assess resistance rate and related factors.
Results: Eighty-four patients were included in the study (18 patients were receiving MTX and 66 patients were receiving ActD). 85.7% of all participants achieved complete remission after first-line chemotherapy (72.2% in MTX vs 89.4% in ActD). There was a significant association for higher tumor size (P=0.046), the occurrence of metastasis (P=0.019), and pretreatment β-HCG levels (P=0.005) with resistance to treatment.
Conclusion: This study demonstrated higher tumor size, the occurrence of metastasis, and pretreatment β-HCG levels have been associated with increased resistance to first-line chemotherapy agents.
Keywords: Dactinomycin; Gestational trophoblastic neoplasia; Methotrexate; Single-agent chemotherapy; Treatment failure.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Goldstein DP, Berkowitz RS, Horowitz NS. Optimal management of low-risk gestational trophoblastic neoplasia. Expert Rev Anticancer Ther. 2015;15:1293–304. - PubMed
-
- Gockley AA, Joseph NT, Melamed A, et al. Effect of race/ethnicity on clinical presentation and risk of gestational trophoblastic neoplasia in patients with complete and partial molar pregnancy at a tertiary care referral center. Am J Obstet Gynecol. 2016;215:334.e1–6. - PubMed
LinkOut - more resources
Full Text Sources