

Short-term Results of Hemiarthroplasty of the Ankle Joint for Talar-Sided Cartilage Loss
- PMID: 36741679
- PMCID: PMC9893082
- DOI: 10.1177/24730114221148172
Short-term Results of Hemiarthroplasty of the Ankle Joint for Talar-Sided Cartilage Loss
Abstract
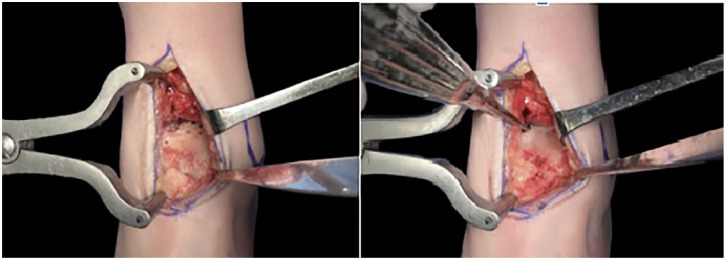
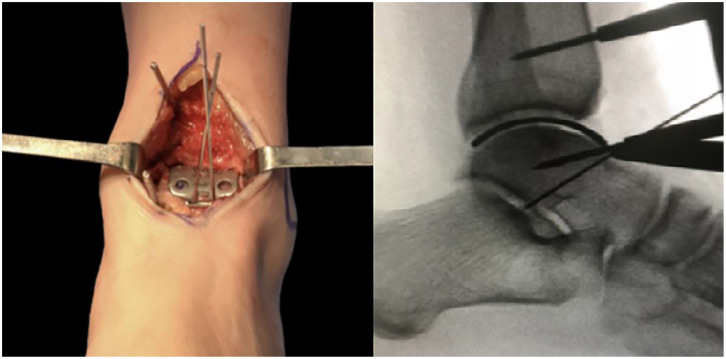
Background: Ankle hemiarthroplasty is a 1-piece implant system replacing the talar side of the tibiotalar joint. Hemiarthroplasty offers limited bone resection and may provide easier revision options than joint-ablating procedures.
Methods: Prospective, multicenter, noncomparative, nonrandomized clinical study with short term follow-up on patients undergoing hemiarthroplasty of the ankle. Radiologic and functional outcomes (Foot and Ankle Outcome Score FAOS, Foot and Ankle Ability Measure [FAAM], Short Form-36 Health Survey [SF-36], Short Musculoskeletal Functional Assessment [SMFA], and visual analog scale [VAS] pain scores) were obtained at 3 and 12 months and the last follow-up (mean 31.9 months).
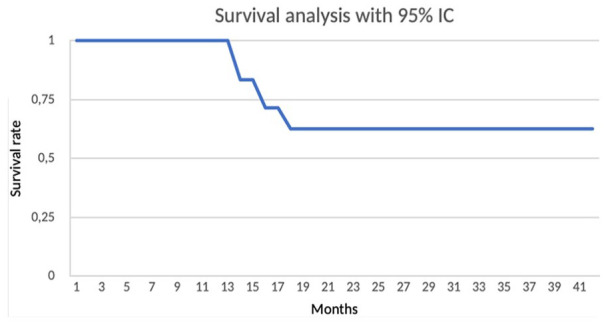
Results: Ten patients met the inclusion criteria. Three were converted to total ankle replacement at 14, 16, and 18 months. Pain VAS scores improved on average from 6.8 to 4.8 (P = .044) of the remaining 7 at a mean of 31.9 months' follow-up. For these 7 in the Survival Group, we found that SF-36 physical health component improved from 25.03 to 42.25 (P = .030), SMFA dysfunction and bother indexes improved from 46.36 to 32.28 (P = .001), and from 55.21 to 30.14 (P = .002) in the Survival Group, and FAAM sports improved from 12.5 to 34.5 (P = .023).
Conclusion: Patients undergoing hemiarthroplasty of the ankle joint for talar-sided lesions had a 30% failure rate by 18 months. Those who did not have an early failure exhibited modest pain reduction, functional improvements, and better quality of life in short-term follow-up. This procedure offers a possible alternative for isolated talar ankle cartilage cases.
Level of evidence: Level IV, prospective case series.
Keywords: ankle arthritis; ankle spacer; hemiarthroplasty; osteochondral lesion.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Manuel J. Pellegrini, MD, reports consulting fees from Arthrex. Giovanni Carcuro, MD, reports consulting fees and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Arthrex. ICMJE forms for all authors are available online.
Figures




References
-
- Adams SB, Viens NA, Easley ME, Stinnett SS, Nunley JA. Midterm results of osteochondral lesions of the talar shoulder treated with fresh osteochondral allograft transplantation. J Bone Joint Surg Am. 2011;93(7):648-654. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous