

Enteral Feeding for Children on Bilevel Positive Pressure Ventilation for Status Asthmaticus
- PMID: 36742255
- PMCID: PMC9894693
- DOI: 10.1055/s-0041-1730901
Enteral Feeding for Children on Bilevel Positive Pressure Ventilation for Status Asthmaticus
Abstract
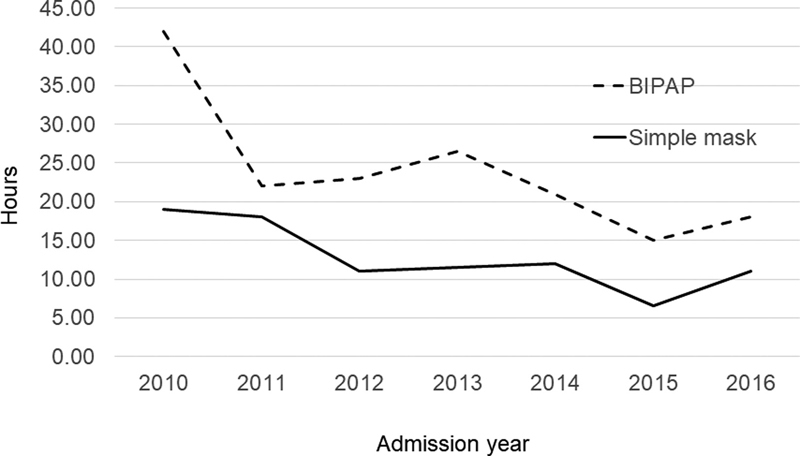
A retrospective data analysis was conducted to evaluate enteral nutrition practices for children admitted with status asthmaticus in a single-center pediatric intensive care unit. Of 406 charts, 315 were analyzed (63% male); 135 on bilevel positive airway pressure ventilation (BIPAP) and 180 on simple mask. Overall median age and weight were 6.0 (interquartile range [IQR]: 6.0) years and 24.8 (IQR: 20.8) kg, respectively. All children studied were on full feeds while still on BIPAP and simple mask; 99.3 and 100% were fed per oral, respectively. Median time to initiation of feeds and full feeds was longer in the BIPAP group, 11.0 (IQR: 20) and 23.0 hours (IQR: 26), versus simple mask group, 4.3 (IQR: 7) and 12.0 hours (IQR: 15), p = 0.001. The results remained similar after adjusting for gender, weight, clinical asthma score at admission, use of adjunct therapy, and duration of continuous albuterol. By 24 hours, 81.5% of patients on BIPAP and 96.6% on simple mask were started on feeds. Compared with simple mask, patients on BIPAP were sicker with median asthma score at admission of 4 (IQR: 2) versus 3 (IQR: 2) on simple mask, requiring more adjunct therapy (80.0 vs. 43.9%), and a longer median length of therapy of 41.0 (IQR: 41) versus 20.0 hours (IQR: 29), respectively, p = 0.001. There were no complications such as aspiration pneumonia, and none required invasive mechanical ventilation in either group. Enteral nutrition was effectively and safely initiated and continued for children admitted with status asthmaticus, including those on noninvasive bilevel ventilation therapy.
Keywords: asthma; bilevel positive pressure ventilation; enteral nutrition; noninvasive ventilation; pediatric; status asthmaticus.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures

References
-
- American Lung Association Asthma and children fact sheetAccessed April 16, 2021 at:https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/lea...
-
- Basnet S, Mander G, Andoh J, Klaska H, Verhulst S, Koirala J. Safety, efficacy, and tolerability of early initiation of noninvasive positive pressure ventilation in pediatric patients admitted with status asthmaticus: a pilot study. Pediatr Crit Care Med. 2012;13(04):393–398. - PubMed
LinkOut - more resources
Full Text Sources