

Endoscopic Adenoidectomy Replacing the Outdated Curette Adenoidectomy: Comparison of the Two Methods at a Tertiary Care Centre
- PMID: 36742736
- PMCID: PMC9895188
- DOI: 10.1007/s12070-022-03089-y
Endoscopic Adenoidectomy Replacing the Outdated Curette Adenoidectomy: Comparison of the Two Methods at a Tertiary Care Centre
Abstract
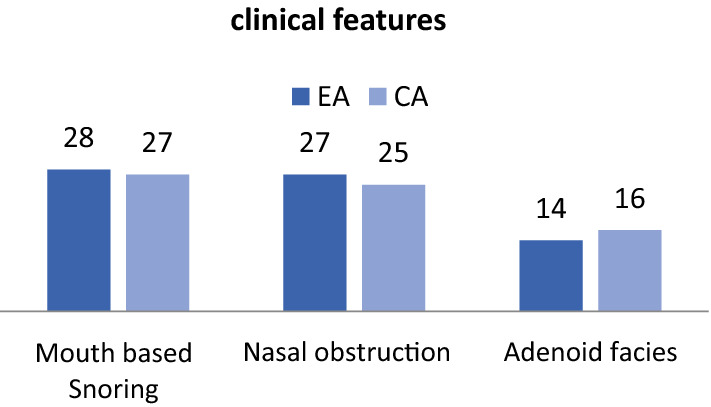
To compare intraoperative and postoperative parameters of the two techniques of adenoidectomy, endoscope and microdebrider powered adenoidectomy and conventional adenoidectomy. Study Design Prospective study. Setting: Academic tertiary referral centre. In our study, cases of adenoid hypertrophy were randomly selected from the outpatient department of department of ORL & HNS. Out of these patients, 30 underwent Endoscopic adenoidectomy (EA) (Group A) and 30 underwent Conventional adenoidectomy (CA) (Group B). All of the patients were assessed pre-operatively, intra-operatively and post-operatively to compare the various parameters. The most common complaint in both the groups was mouth breathing with snoring. Intra-operative bleeding was 29.15 ml in group EA and 15.2 ml in group CA. Operative time for CA was shorter at 21.8 min as compared to 32.1 min for group EA. Residual adenoids and injury to adjacent structures were more common in group CA. Hospital stay was 3.2 days for EA patients and 3.43 days for CA patients. Resolution of symptoms was near comparable in both groups. Operative time and intra-operative bleeding are both significantly reduced with the CA as opposed to EA. However, injury to adjacent structures and residual adenoids occur significantly less in group EA. After weighing the risks and benefits, we can conclude that EA is comparatively better than CA.
Keywords: Adenoidectomy; Adenoids; Curette; Endoscopic; Microdebrider; Operative time; Surgical outcome.
© Association of Otolaryngologists of India 2022.
Conflict of interest statement
Conflict of interestThe authors declare that they have no financial interest.
Figures






References
LinkOut - more resources
Full Text Sources