

Trifluridine/tipiracil with or without bevacizumab in metastatic colorectal cancer: results of a systematic review and meta-analysis
- PMID: 36743525
- PMCID: PMC9893398
- DOI: 10.1177/17588359221146137
Trifluridine/tipiracil with or without bevacizumab in metastatic colorectal cancer: results of a systematic review and meta-analysis
Abstract
Background: Trifluridine/tipiracil plus bevacizumab (FTD/TPI + BEV) has shown efficacy and tolerability in refractory metastatic colorectal cancer (mCRC). Because randomized controlled trial (RCT) data comparing FTD/TPI + BEV with FTD/TPI are lacking, this meta-analysis evaluated outcomes with both regimens.
Data sources and methods: Electronic databases, congress proceedings (past 3 years), trial registries, systematic review bibliographies, gray literature, and guidelines through June 2021 were searched for RCTs, non-RCTs, and prospective observational studies involving >20 previously treated patients with mCRC receiving FTD/TPI + BEV or FTD/TPI. Absolute and relative disease control rate (DCR), progression-free survival (PFS), overall survival (OS), adverse event (AE) rates, and discontinuation rates due to AEs were evaluated using fixed-effects and random-effects models. Study quality, heterogeneity, and publication bias were assessed.
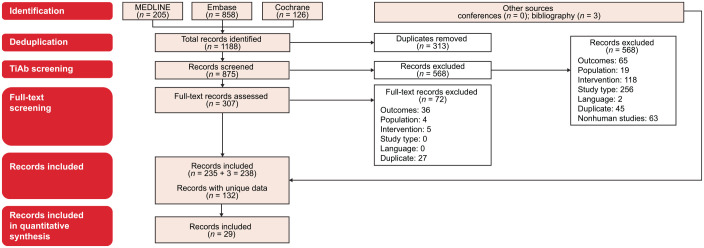
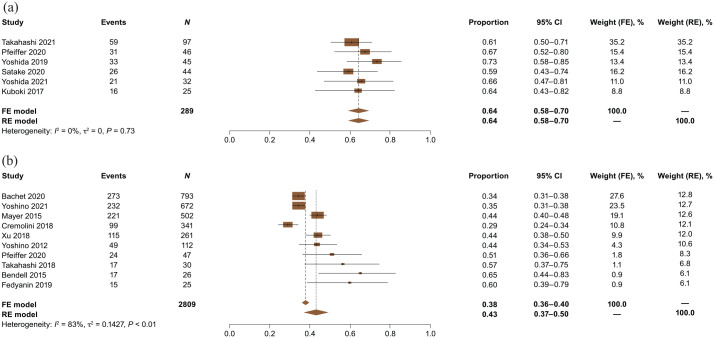
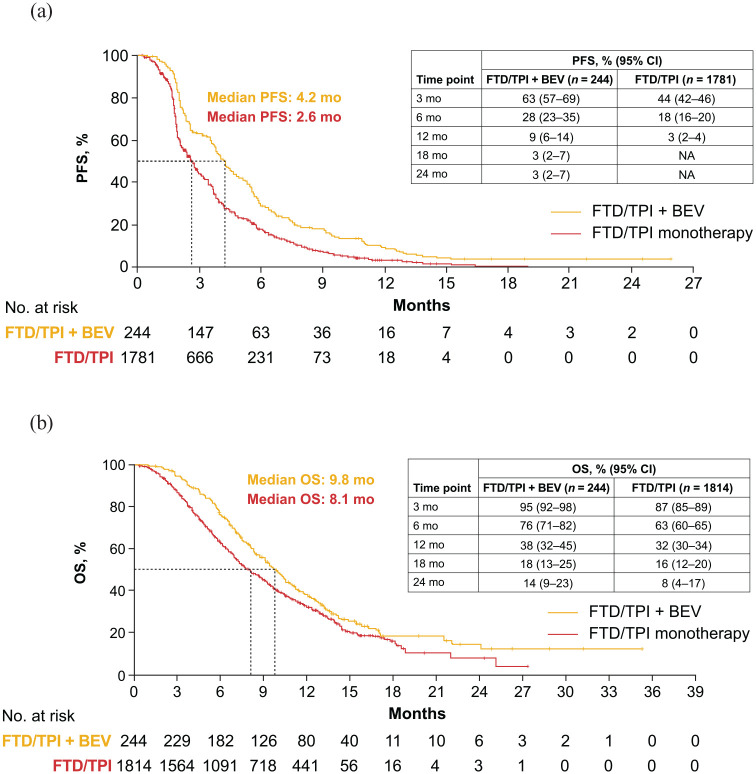
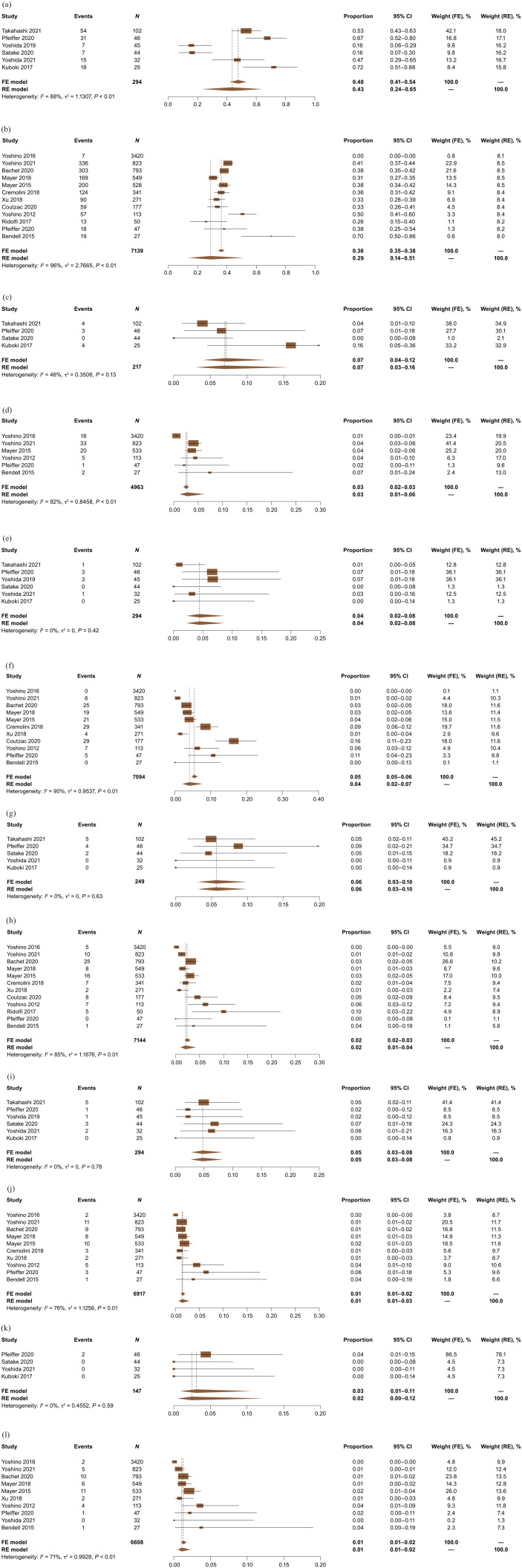
Results: In all, 29 of 875 screened publications were selected (26 studies: 5 RCTs, 11 non-RCTs, and 10 prospective observational studies). One RCT compared FTD/TPI + BEV with FTD/TPI. FTD/TPI + BEV versus FTD/TPI had a higher absolute DCR [64% (6 studies; n = 289) versus 43% (10 studies; n = 2809)], median PFS [4.2 (5 studies; n = 244) versus 2.6 (6 studies; n = 1781) months], 12-month PFS [9% (5 studies; n = 244) versus 3% (6 studies; n = 1781)], median OS [9.8 (5 studies; n = 244) versus 8.1 (6 studies; n = 1814) months], and 12-month OS [38% (5 studies; n = 244) versus 32% (6 studies; n = 1814)]. Grade ⩾3 febrile neutropenia, asthenia/fatigue, diarrhea, nausea, and vomiting rates were similar (1%-7%). Grade ⩾3 neutropenia rate was higher with FTD/TPI + BEV than with FTD/TPI [43% (6 studies; n = 294) versus 29% (12 studies; n = 7139)]. Discontinuation rates due to AEs were similar [8% (5 studies; n = 244) and 7% (10 studies; n = 3724)]. Low study quality, heterogeneity, and/or publication bias were detected in certain instances.
Conclusion: Despite fewer patients treated with the combination, this meta-analysis consistently suggested that FTD/TPI + BEV provides benefits over FTD/TPI in refractory mCRC and has similar safety, except for more frequent grade ⩾3 neutropenia.
Keywords: bevacizumab; meta-analysis; metastatic colorectal cancer; overall survival; progression-free survival; safety; trifluridine/tipiracil.
© The Author(s), 2023.
Conflict of interest statement
Takayuki Yoshino reports medical writing support for the submitted work from Taiho Oncology; lecture fees and/or honoraria from Bayer Yakuhin, MSD K.K., Chugai Pharmaceutical, Eli Lilly Japan K.K, Merck Biopharma, Ono Pharmaceutical, and Taiho Pharmaceutical; research funds to his institution from Amgen K.K., Pfizer Japan, Chugai Pharmaceutical, Genomedia, MSD K.K., Nippon Boehringer Ingelheim, Ono Pharmaceutical, Parexel International, Sanofi K.K, Daiichi Sankyo, Sysmex Corporation, and Taiho Pharmaceutical. Julien Taieb reports medical writing support for the submitted work from Taiho Oncology; consulting fees, payment or honoraria, and support for attending meetings and/or travel from Amgen, Astellas, AstraZeneca, Bristol Myers Squibb, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, and Servier. Yasutoshi Kuboki reports medical writing support for the submitted work from Taiho Oncology; grants or contracts Abbie, Astelas, AstraZeneca, Boehringer Ingelheim, Chugai, Daiichi-Sankyo, Genmab, GlaxoSmithKline, Incyte, Lilly, Taiho Oncology, and Takeda; consulting fees from Amgen, Boehringer Ingelheim, Taiho, and Takeda; payment or honoraria from Bristol Myers Squibb, Lilly, Ono, and Taiho Oncology. Per Pfeiffer reports medical writing support for the submitted work from Taiho Oncology and grants to his institution from Servier. Amit Kumar reports medical writing support for the submitted work from Taiho Oncology and is an employee of SmartAnalyst, the consulting firm contracted by Taiho Oncology to conduct the analysis for the submitted work and by Bristol Myers Squibb, Janssen, Pfizer, and Merck for unrelated work. Howard S. Hochster reports medical writing support for the submitted work and payment for expert testimony from Taiho Oncology, Inc.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al.. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. - PubMed
-
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: colorectal cancer, https://seer.cancer.gov/statfacts/html/colorect.html (2022, accessed 18 February 2022).
-
- Van Cutsem E, Cervantes A, Adam R, et al.. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol 2016; 27: 1386–1422. - PubMed
-
- Biller LH, Schrag D. Diagnosis and treatment of metastatic colorectal cancer: a review. JAMA 2021; 325: 669–685. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
