

The therapeutic threshold in clinical decision-making for TB
- PMID: 36744621
- PMCID: PMC10629962
- DOI: 10.1093/inthealth/ihad002
The therapeutic threshold in clinical decision-making for TB
Abstract
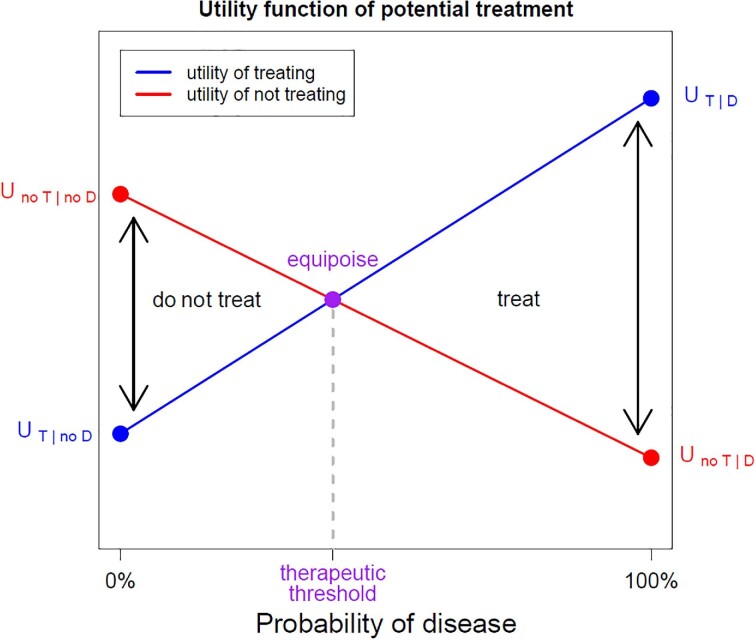
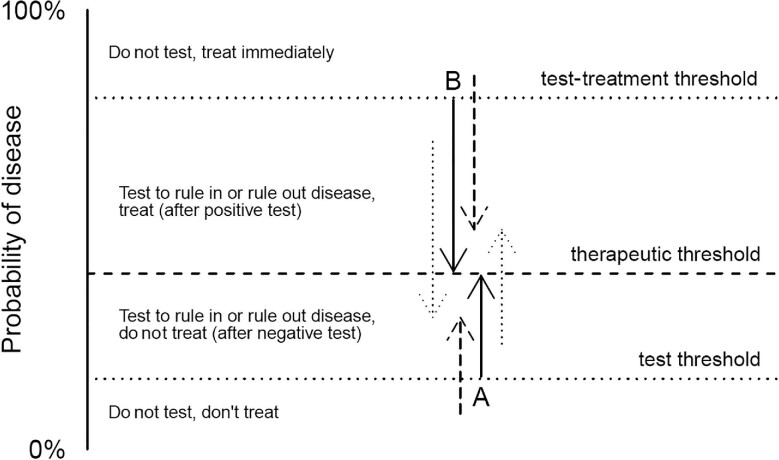
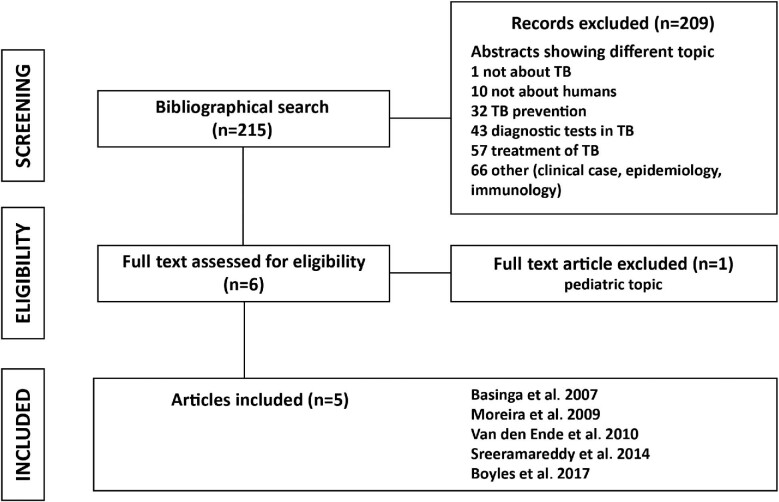
Because TB control is still hampered by the limitations of diagnostic tools, diagnostic uncertainty is common. The decision to offer treatment is based on clinical decision-making. The therapeutic threshold, test threshold and test-treatment threshold can guide in making these decisions. This review summarizes the literature on methods to estimate the therapeutic threshold that have been applied for TB. Only five studies estimated the threshold for the diagnosis of TB. The therapeutic threshold can be estimated by prescriptive methods, based on calculations, and by descriptive methods, deriving the threshold from observing clinical practice. Test and test-treatment thresholds can be calculated using the therapeutic threshold and the characteristics of an available diagnostic test. Estimates of the therapeutic threshold for pulmonary TB from intuitive descriptive approaches (20%-50%) are higher than theoretical prescriptive calculations (2%-3%). In conclusion, estimates of the therapeutic threshold for pulmonary TB depend on the method used. Other methods exist within the field of decision-making that have yet to be implemented or adapted as tools to estimate the TB therapeutic threshold. Because clinical decision-making is a core element of TB management, it is necessary to find a new, clinician-friendly way to unbiasedly estimate context-specific, agreed upon therapeutic thresholds.
Keywords: TB; clinical decision-making; diagnosis; threshold.
© The Author(s) 2023. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene.
Conflict of interest statement
All authors declare no conflict of interests.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2020. World Heal Organ. 2020:232.
-
- Zifodya JS, Kreniske JS, Schiller Iet al. . Xpert Ultra versus Xpert MTB/RIF for pulmonary tuberculosis and rifampicin resistance in adults with presumptive pulmonary tuberculosis. Cochrane Database Syst Rev. 2021;2021(2). - PubMed
-
- Sox HC, Higgins MC, Owens DK. Medical Decision Making. Chichester, UK: John Wiley and Sons; 2013.
-
- Pauker SG, Kassirer JP.. Therapeutic decision making: A cost-benefit analysis. N Engl J Med. 1975;293(5):229–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
