

Providing Human Support for the Use of Digital Mental Health Interventions: Systematic Meta-review
- PMID: 36745497
- PMCID: PMC9941905
- DOI: 10.2196/42864
Providing Human Support for the Use of Digital Mental Health Interventions: Systematic Meta-review
Abstract
Background: Digital mental health interventions (DMHIs) have been increasingly deployed to bridge gaps in mental health care, particularly given their promising efficacy. Nevertheless, attrition among DMHI users remains high. In response, human support has been studied as a means of improving retention to and outcomes of DMHIs. Although a growing number of studies and meta-analyses have investigated the effects of human support for DMHIs on mental health outcomes, systematic empirical evidence of its effectiveness across mental health domains remains scant.
Objective: We aimed to summarize the results of meta-analyses of human support versus no support for DMHI use across various outcome domains, participant samples, and support providers.
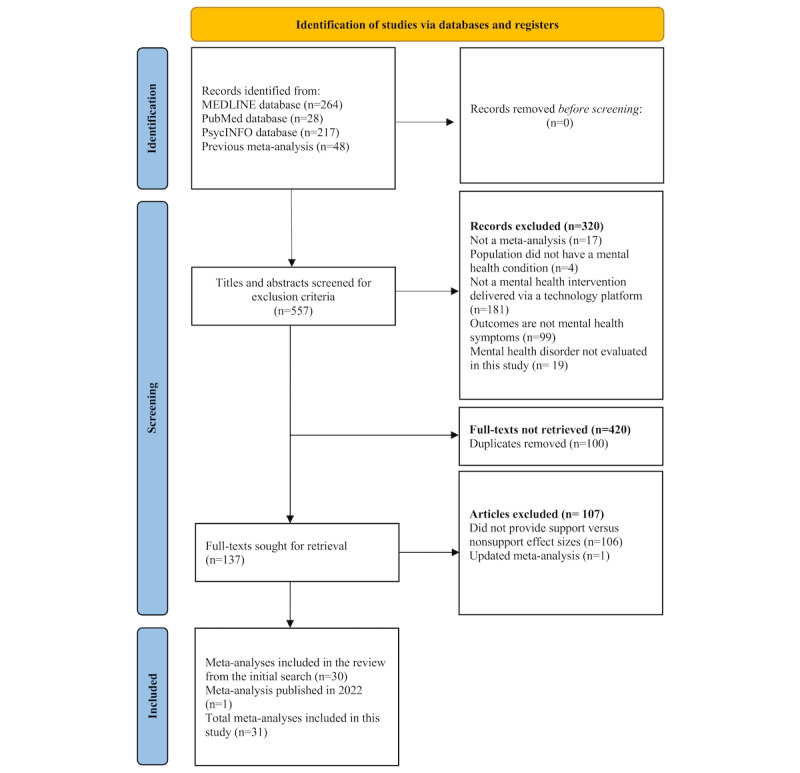
Methods: We conducted a systematic meta-review of meta-analyses, comparing the effects of human support with those of no support for DMHI use, with the goal of qualitatively summarizing data across various outcome domains, participant samples, and support providers. We used MEDLINE, PubMed, and PsycINFO electronic databases. Articles were included if the study had a quantitative meta-analysis study design; the intervention targeted mental health symptoms and was delivered via a technology platform (excluding person-delivered interventions mediated through telehealth, text messages, or social media); the outcome variables included mental health symptoms such as anxiety, depression, stress, posttraumatic stress disorder symptoms, or a number of these symptoms together; and the study included quantitative comparisons of outcomes in which human support versus those when no or minimal human support was provided.
Results: The results of 31 meta-analyses (505 unique primary studies) were analyzed. The meta-analyses reported 45 effect sizes; almost half (n=22, 48%) of them showed that human-supported DMHIs were significantly more effective than unsupported DMHIs. A total of 9% (4/45) of effect sizes showed that unsupported DMHIs were significantly more effective. No clear patterns of results emerged regarding the efficacy of human support for the outcomes assessed (including anxiety, depression, posttraumatic stress disorder, stress, and multiple outcomes). Human-supported DMHIs may be more effective than unsupported DMHIs for individuals with elevated mental health symptoms. There were no clear results regarding the type of training for those providing support.
Conclusions: Our findings highlight the potential of human support in improving the effects of DMHIs. Specifically, evidence emerged for stronger effects of human support for individuals with greater symptom severity. There was considerable heterogeneity across meta-analyses in the level of detail regarding the nature of the interventions, population served, and support delivered, making it difficult to draw strong conclusions regarding the circumstances under which human support is most effective. Future research should emphasize reporting detailed descriptions of sample and intervention characteristics and describe the mechanism through which they believe the coach will be most useful for the DMHI.
Keywords: digital mental health interventions; human support; supportive accountability; systematic meta-review.
©Alexandra Werntz, Selen Amado, Megyn Jasman, Ariel Ervin, Jean E Rhodes. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 06.02.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
References
-
- Liverpool S, Mota CP, Sales CM, Čuš A, Carletto S, Hancheva C, Sousa S, Cerón SC, Moreno-Peral P, Pietrabissa G, Moltrecht B, Ulberg R, Ferreira N, Edbrooke-Childs J. Engaging children and young people in digital mental health interventions: systematic review of modes of delivery, facilitators, and barriers. J Med Internet Res. 2020 Jun 23;22(6):e16317. doi: 10.2196/16317. http://hdl.handle.net/2318/1742226 v22i6e16317 - DOI - PMC - PubMed
-
- West R, Michie S. A Guide to Development and Evaluation of Digital Behaviour Change Interventions in Healthcare. Sutton, UK: Silverback Publishing; 2016.
-
- Rauschenberg C, Schick A, Hirjak D, Seidler A, Paetzold I, Apfelbacher C, Riedel-Heller SG, Reininghaus U. Evidence synthesis of digital interventions to mitigate the negative impact of the COVID-19 pandemic on public mental health: rapid meta-review. J Med Internet Res. 2021 Mar 10;23(3):e23365. doi: 10.2196/23365. https://www.jmir.org/2021/3/e23365/ v23i3e23365 - DOI - PMC - PubMed
-
- Heber E, Ebert DD, Lehr D, Cuijpers P, Berking M, Nobis S, Riper H. The benefit of web- and computer-based interventions for stress: a systematic review and meta-analysis. J Med Internet Res. 2017 Feb 17;19(2):e32. doi: 10.2196/jmir.5774. https://www.jmir.org/2017/2/e32/ v19i2e32 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
