

A unified classification approach rating clinical utility of protein biomarkers across neurologic diseases
- PMID: 36745974
- PMCID: PMC9931915
- DOI: 10.1016/j.ebiom.2023.104456
A unified classification approach rating clinical utility of protein biomarkers across neurologic diseases
Abstract
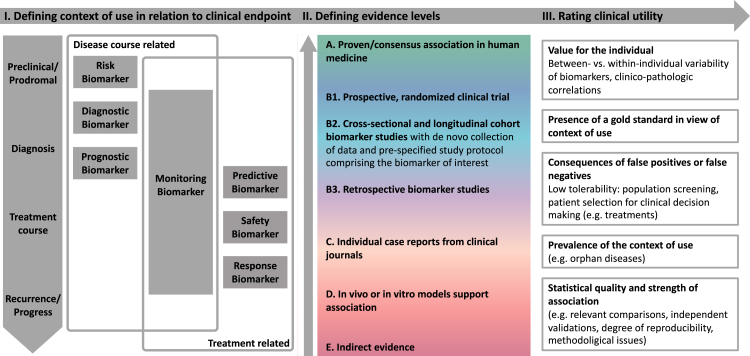
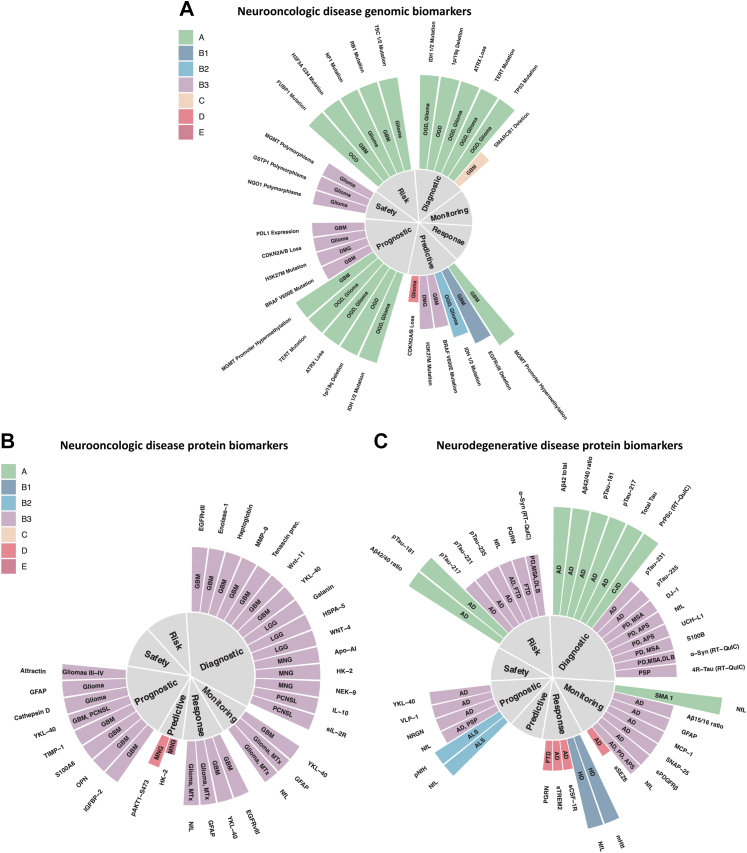
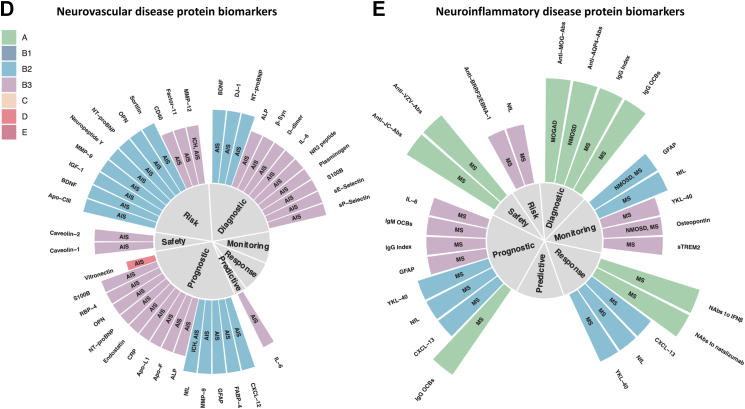
A major evolution from purely clinical diagnoses to biomarker supported clinical diagnosing has been occurring over the past years in neurology. High-throughput methods, such as next-generation sequencing and mass spectrometry-based proteomics along with improved neuroimaging methods, are accelerating this development. This calls for a consensus framework that is broadly applicable and provides a spot-on overview of the clinical validity of novel biomarkers. We propose a harmonized terminology and a uniform concept that stratifies biomarkers according to clinical context of use and evidence levels, adapted from existing frameworks in oncology with a strong focus on (epi)genetic markers and treatment context. We demonstrate that this framework allows for a consistent assessment of clinical validity across disease entities and that sufficient evidence for many clinical applications of protein biomarkers is lacking. Our framework may help to identify promising biomarker candidates and classify their applications by clinical context, aiming for routine clinical use of (protein) biomarkers in neurology.
Keywords: Analytical validity; Biomarker; Clinical utility; Neurology; Protein; Proteomics.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests Johannes Levin reports part-time employment by MODAG GmbH and a grant of the Michael J Fox Foundation for Parkinson's Research. In addition, he reports speaker fees from Bayer Vital, Biogen and Roche, consulting fees from Axon Neuroscience and Biogen, author fees from Thieme medical publishers and W. Kohlhammer GmbH medical publishers, all outside the submitted work. He is a member of the advisory board of Biogen and a member of the Data Safety Monitoring Board of Axon Neuroscience. He is beneficiary of the phantom share program of MODAG GmbH. In addition, he is inventor in a patent “Pharmaceutical Composition and Methods of Use” (EP 22 159 408.8) filed by MODAG GmbH. Bernhard Hemmer received funding by the European Union's Horizon 2020 Research and Innovation Program and the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany's Excellence Strategy within the framework of the Munich Cluster for Systems Neurology and Roche. He holds part of two patents: one for the detection of antibodies against KIR4.1 in a subpopulation of patients with multiple sclerosis and one for genetic determinants of neutralizing antibodies to interferon. Wilko Weichert reports research funding from Roche, MSD, BMS and AstraZeneca. He has attended and given talks at Advisory Boards, gave advice to and served as speaker on national and international conferences for Roche, MSD, BMS, AstraZeneca, Pfizer, Merck, Lilly, Boehringer, Novartis, Takeda, Bayer, Amgen, Astellas, Eisai, Johnson and Johnson, Janssen, Illumina, Siemens, Agilent, ADC, GSK and Molecular Health. Stefan F. Lichtenthaler reports research funding from Shionogi and Novartis. Steffen Tiedt reports consulting fees from Alpha Apollo Inc. Christiane Gasperi reports funding from the Hertie Foundation, the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) and the Hans and Klementia Langmatz Stiftung. Carla Palleis reports funding from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany's Excellence Strategy within the framework of the Munich Cluster for Systems Neurology. No other disclosures were reported.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
