

Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation based on image analysis and clinical findings: A retrospective review of 345 cases
- PMID: 36749265
- PMCID: PMC9901959
- DOI: 10.1097/MD.0000000000032832
Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation based on image analysis and clinical findings: A retrospective review of 345 cases
Abstract
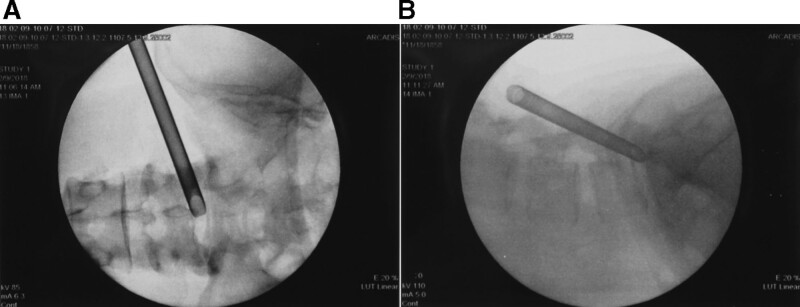
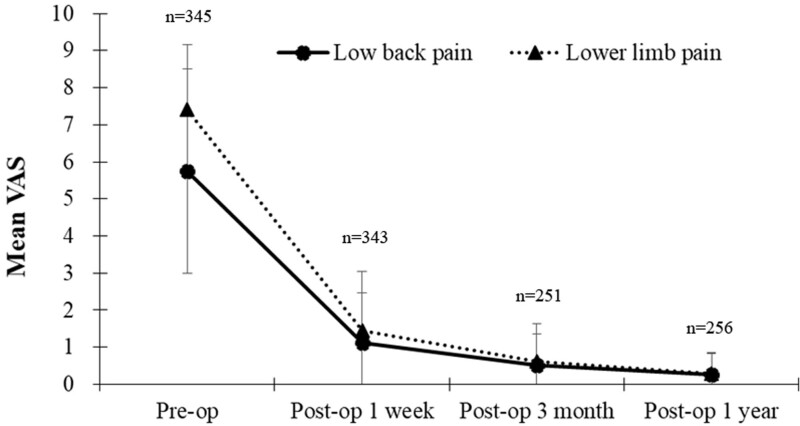
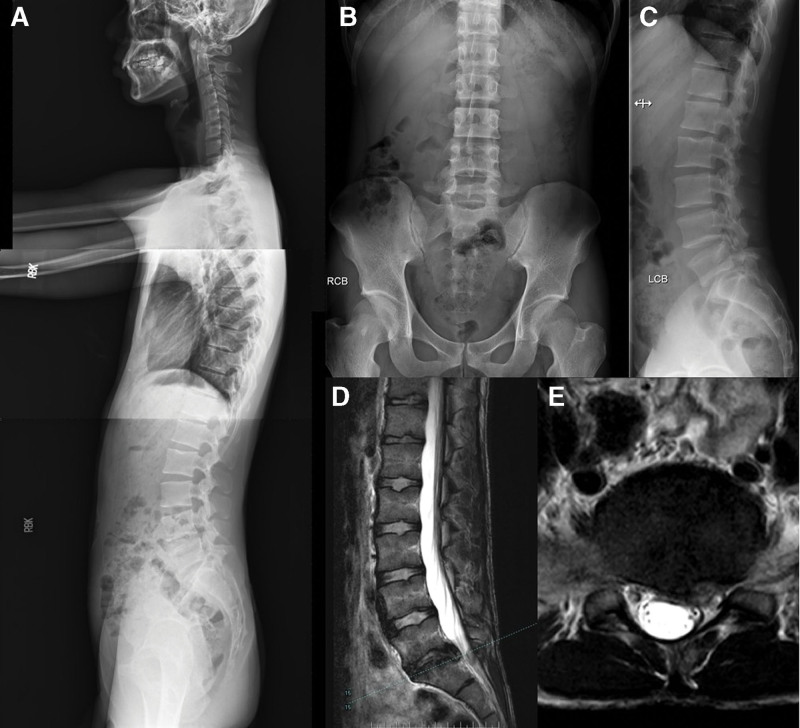
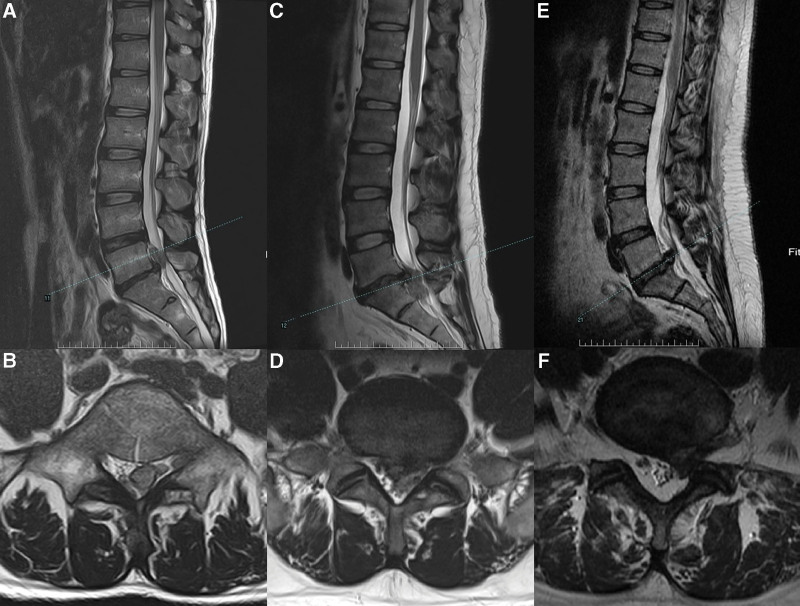
The effect of spinal anatomical anomalies on the efficacy of percutaneous endoscopic lumbar discectomy (PELD) for disc herniation repair is unclear. This retrospective review aims to assess the safety and effectiveness of PELD for treating L5-S1 disc herniation with a range of characteristics and to determine the prevalence of lumbosacral transitional vertebrae (LSTV) anatomical anomalies to facilitate pre-surgical planning. From July 2005 to June 2019, 345 patients with L5-S1 disc herniations were treated with PELD. The primary outcome was 1-year postoperative visual analogue scale scores for low back and lower limb pain. The secondary outcomes included the surgical approach used, lumbosacral bony anomalies, presence of a ruptured disc or severely calcified disc, pediatric lumbar disc herniation, recurrent disc herniation management, and the long-term outcome. visual analogue scale scores for most patients were significantly improved after surgery. The prevalence of LSTVs was 4.05% (14/345 patients) in lumbar sacralization and 7.53% (26/345 patients) in sacral lumbarization. The prevalence of ruptured and severely calcified discs was 18.55% (64/345) and 5.79% (20/345), respectively. The prevalence of pediatric lumbar disc herniation was 2.02% (7/345). The recurrence rate was 4.34% (15/345). Two durotomy cases without sequelae and 8 cases of lower limb dysesthesia lasting longer than 3 months postoperatively were reported. PELD is safe and effective for treating L5-S1 disc herniation, including cases complicated by calcified lumbar disc herniation, disc rupture with migration, and the presence of LSTV. Appropriate imaging is essential to identify case-specific factors, including the prevalent LSTV anatomical anomalies, before surgery.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Ozer AF, Oktenoglu T, Sasani M, et al. Preserving the ligamentum flavum in lumbar discectomy: a new technique that prevents scar tissue formation in the first 6 months postsurgery. Neurosurgery. 2006;59:ONS126–33. - PubMed
-
- Slotkin JR, Mislow JM, Day AL, et al. Pediatric disk disease. Neurosurg Clin N Am. 2007;18:659–67. - PubMed
-
- Wang X, Zeng J, Nie H, et al. Percutaneous endoscopic interlaminar discectomy for pediatric lumbar disc herniation. Childs Nerv Syst. 2014;30:897–902. - PubMed
-
- Delport EG, Cucuzzella TR, Kim N, et al. Lumbosacral transitional vertebrae: incidence in a consecutive patient series. Pain Physician. 2006;9:53–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
