

Four-Year Visual Outcomes in the Protocol W Randomized Trial of Intravitreous Aflibercept for Prevention of Vision-Threatening Complications of Diabetic Retinopathy
- PMID: 36749332
- PMCID: PMC10408259
- DOI: 10.1001/jama.2022.25029
Four-Year Visual Outcomes in the Protocol W Randomized Trial of Intravitreous Aflibercept for Prevention of Vision-Threatening Complications of Diabetic Retinopathy
Erratum in
-
Incorrect Data in Abstract and Figure.JAMA. 2023 Mar 28;329(12):1034. doi: 10.1001/jama.2023.3272. JAMA. 2023. PMID: 36976291 Free PMC article. No abstract available.
Abstract
Importance: Anti-vascular endothelial growth factor (VEGF) injections in eyes with nonproliferative diabetic retinopathy (NPDR) without center-involved diabetic macular edema (CI-DME) reduce development of vision-threatening complications from diabetes over at least 2 years, but whether this treatment has a longer-term benefit on visual acuity is unknown.
Objective: To compare the primary 4-year outcomes of visual acuity and rates of vision-threatening complications in eyes with moderate to severe NPDR treated with intravitreal aflibercept compared with sham. The primary 2-year analysis of this study has been reported.
Design, setting, and participants: Randomized clinical trial conducted at 64 clinical sites in the US and Canada from January 2016 to March 2018, enrolling 328 adults (399 eyes) with moderate to severe NPDR (Early Treatment Diabetic Retinopathy Study [ETDRS] severity level 43-53; range, 0 [worst] to 100 [best]) without CI-DME.
Interventions: Eyes were randomly assigned to 2.0 mg aflibercept (n = 200) or sham (n = 199). Eight injections were administered at defined intervals through 2 years, continuing quarterly through 4 years unless the eye improved to mild NPDR or better. Aflibercept was given in both groups to treat development of high-risk proliferative diabetic retinopathy (PDR) or CI-DME with vision loss.
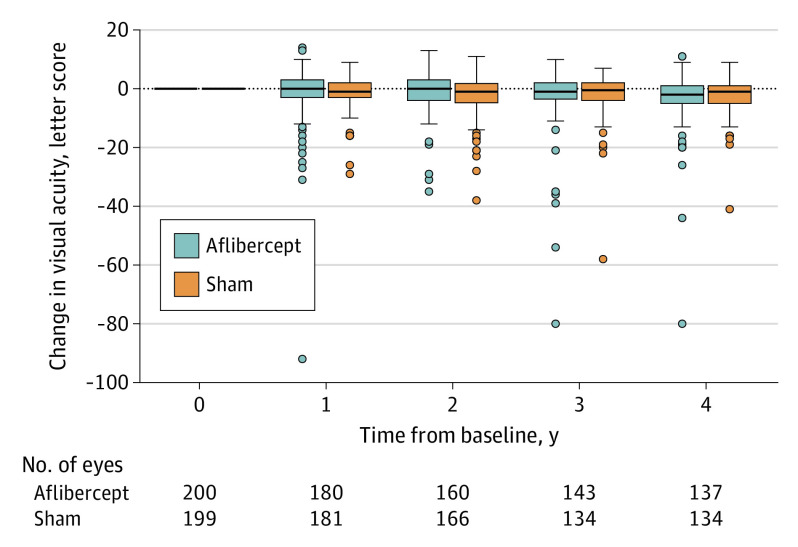
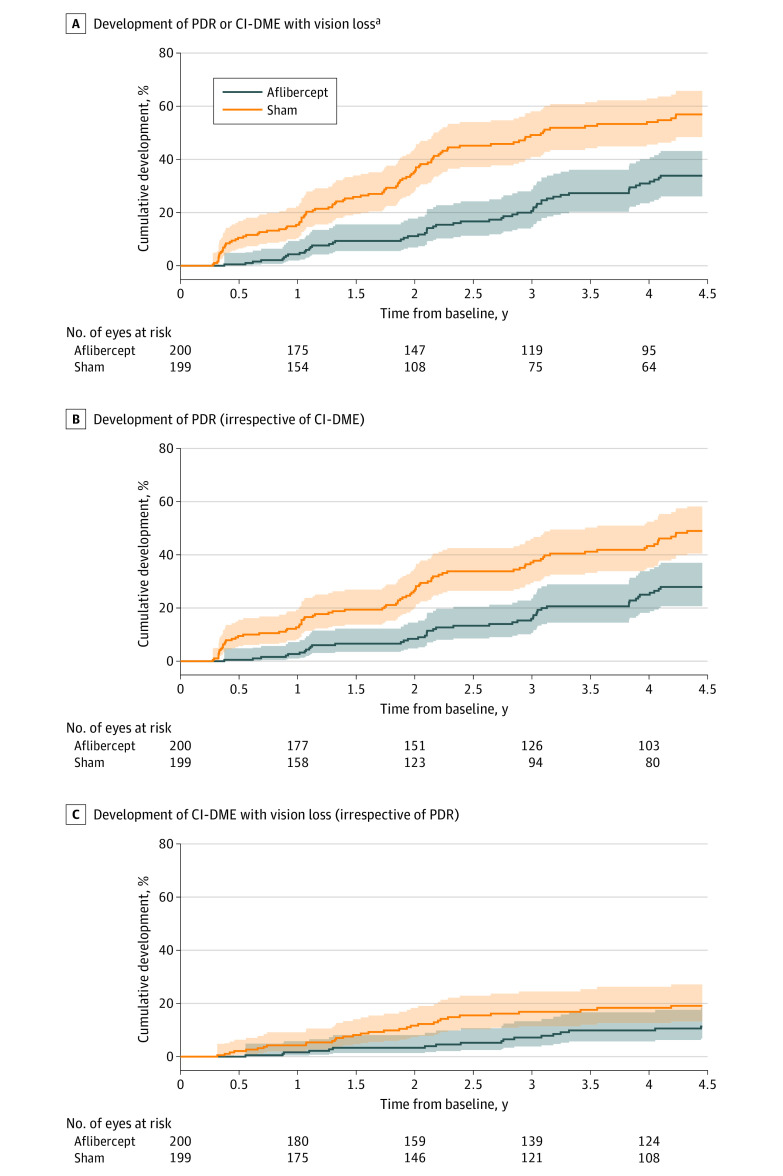
Main outcomes and measures: Development of PDR or CI-DME with vision loss (≥10 letters at 1 visit or ≥5 letters at 2 consecutive visits) and change in visual acuity (best corrected ETDRS letter score) from baseline to 4 years.
Results: Among participants (mean age 56 years; 42.4% female; 5% Asian, 15% Black, 32% Hispanic, 45% White), the 4-year cumulative probability of developing PDR or CI-DME with vision loss was 33.9% with aflibercept vs 56.9% with sham (adjusted hazard ratio, 0.40 [97.5% CI, 0.28 to 0.57]; P < .001). The mean (SD) change in visual acuity from baseline to 4 years was -2.7 (6.5) letters with aflibercept and -2.4 (5.8) letters with sham (adjusted mean difference, -0.5 letters [97.5% CI, -2.3 to 1.3]; P = .52). Antiplatelet Trialists' Collaboration cardiovascular/cerebrovascular event rates were 9.9% (7 of 71) in bilateral participants, 10.9% (14 of 129) in unilateral aflibercept participants, and 7.8% (10 of 128) in unilateral sham participants.
Conclusions and relevance: Among patients with NPDR but without CI-DME at 4 years treatment with aflibercept vs sham, initiating aflibercept treatment only if vision-threatening complications developed, resulted in statistically significant anatomic improvement but no improvement in visual acuity. Aflibercept as a preventive strategy, as used in this trial, may not be generally warranted for patients with NPDR without CI-DME.
Trial registration: ClinicalTrials.gov Identifier: NCT02634333.
Conflict of interest statement
Figures

Comment in
-
Anti-Vascular Endothelial Growth Factor Therapy for Complications of Diabetic Retinopathy-From Treatment to Prevention?JAMA Ophthalmol. 2023 Mar 1;141(3):223-225. doi: 10.1001/jamaophthalmol.2023.0496. JAMA Ophthalmol. 2023. PMID: 36749591 No abstract available.
-
Four-Year Visual Outcomes After Intravitreous Aflibercept for Vision-Threatening Complications of Diabetic Retinopathy.JAMA. 2023 May 23;329(20):1795-1796. doi: 10.1001/jama.2023.6712. JAMA. 2023. PMID: 37219557 No abstract available.
References
-
- Maturi RK, Glassman AR, Josic K, et al. ; DRCR Retina Network . Effect of intravitreous anti-vascular endothelial growth factor vs sham treatment for prevention of vision-threatening complications of diabetic retinopathy: the Protocol W randomized clinical trial. JAMA Ophthalmol. 2021;139(7):701-712. doi: 10.1001/jamaophthalmol.2021.0606 - DOI - PMC - PubMed
-
- Gross JG, Glassman AR, Liu D, et al. ; Diabetic Retinopathy Clinical Research Network . Five-year outcomes of panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA Ophthalmol. 2018;136(10):1138-1148. doi: 10.1001/jamaophthalmol.2018.3255 - DOI - PMC - PubMed
-
- Wells JA, Glassman AR, Ayala AR, et al. ; Diabetic Retinopathy Clinical Research Network . Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123(6):1351-1359. doi: 10.1016/j.ophtha.2016.02.022 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
