

Circulation of Rhinoviruses and/or Enteroviruses in Pediatric Patients With Acute Respiratory Illness Before and During the COVID-19 Pandemic in the US
- PMID: 36749589
- PMCID: PMC10408278
- DOI: 10.1001/jamanetworkopen.2022.54909
Circulation of Rhinoviruses and/or Enteroviruses in Pediatric Patients With Acute Respiratory Illness Before and During the COVID-19 Pandemic in the US
Abstract
Importance: Rhinoviruses and/or enteroviruses, which continued to circulate during the COVID-19 pandemic, are commonly detected in pediatric patients with acute respiratory illness (ARI). Yet detailed characterization of rhinovirus and/or enterovirus detection over time is limited, especially by age group and health care setting.
Objective: To quantify and characterize rhinovirus and/or enterovirus detection before and during the COVID-19 pandemic among children and adolescents seeking medical care for ARI at emergency departments (EDs) or hospitals.
Design, setting, and participants: This cross-sectional study used data from the New Vaccine Surveillance Network (NVSN), a multicenter, active, prospective surveillance platform, for pediatric patients who sought medical care for fever and/or respiratory symptoms at 7 EDs or hospitals within NVSN across the US between December 2016 and February 2021. Persons younger than 18 years were enrolled in NVSN, and respiratory specimens were collected and tested for multiple viruses.
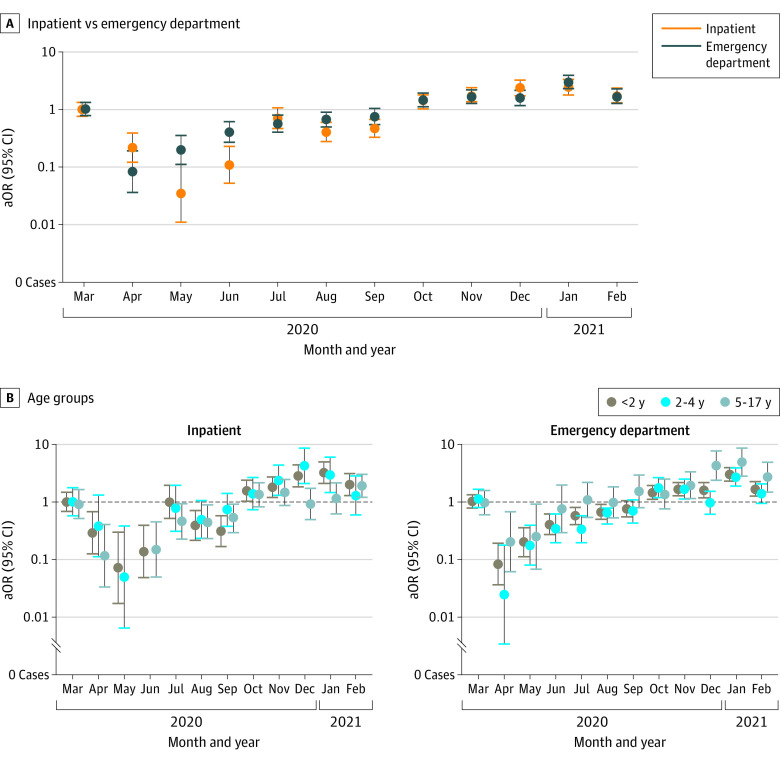
Main outcomes and measures: Proportion of patients in whom rhinovirus and/or enterovirus, or another virus, was detected by calendar month and by prepandemic (December 1, 2016, to March 11, 2020) or pandemic (March 12, 2020, to February 28, 2021) periods. Month-specific adjusted odds ratios (aORs) for rhinovirus and/or enterovirus-positive test results (among all tested) by setting (ED or inpatient) and age group (<2, 2-4, or 5-17 years) were calculated, comparing each month during the pandemic to equivalent months of previous years.
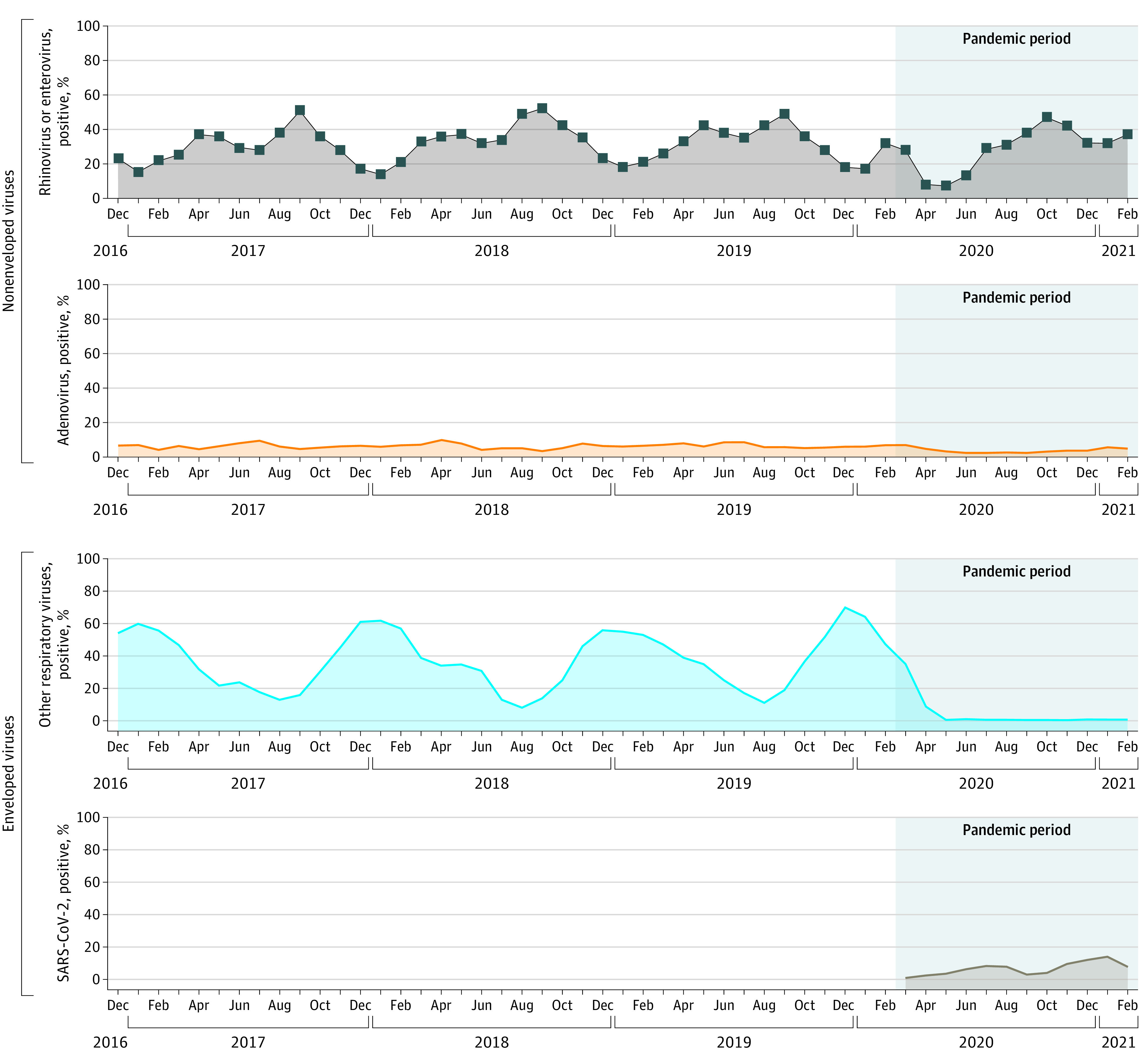
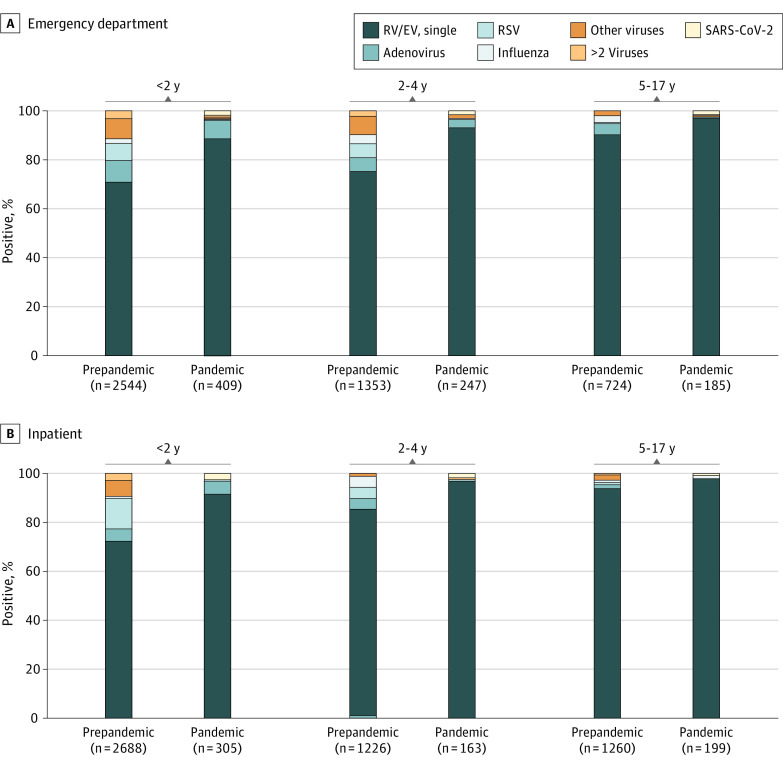
Results: Of the 38 198 children and adolescents who were enrolled and tested, 11 303 (29.6%; mean [SD] age, 2.8 [3.7] years; 6733 boys [59.6%]) had rhinovirus and/or enterovirus-positive test results. In prepandemic and pandemic periods, rhinoviruses and/or enteroviruses were detected in 29.4% (9795 of 33 317) and 30.9% (1508 of 4881) of all patients who were enrolled and tested and in 42.2% (9795 of 23 236) and 73.0% (1508 of 2066) of those with test positivity for any virus, respectively. Rhinoviruses and/or enteroviruses were the most frequently detected viruses in both periods and all age groups in the ED and inpatient setting. From April to September 2020 (pandemic period), rhinoviruses and/or enteroviruses were detectable at similar or lower odds than in prepandemic years, with aORs ranging from 0.08 (95% CI, 0.04-0.19) to 0.76 (95% CI, 0.55-1.05) in the ED and 0.04 (95% CI, 0.01-0.11) to 0.71 (95% CI, 0.47-1.07) in the inpatient setting. However, unlike some other viruses, rhinoviruses and/or enteroviruses soon returned to prepandemic levels and from October 2020 to February 2021 were detected at similar or higher odds than in prepandemic months in both settings, with aORs ranging from 1.47 (95% CI, 1.12-1.93) to 3.01 (95% CI, 2.30-3.94) in the ED and 1.36 (95% CI, 1.03-1.79) to 2.44 (95% CI, 1.78-3.34) in the inpatient setting, and in all age groups. Compared with prepandemic years, during the pandemic, rhinoviruses and/or enteroviruses were detected in patients who were slightly older, although most (74.5% [1124 of 1508]) were younger than 5 years.
Conclusions and relevance: Results of this study show that rhinoviruses and/or enteroviruses persisted and were the most common respiratory virus group detected across all pediatric age groups and in both ED and inpatient settings. Rhinoviruses and/or enteroviruses remain a leading factor in ARI health care burden, and active ARI surveillance in children and adolescents remains critical for defining the health care burden of respiratory viruses.
Conflict of interest statement
Figures
References
-
- Marriott D, Beresford R, Mirdad F, et al. Concomitant marked decline in prevalence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and other respiratory viruses among symptomatic patients following public health interventions in Australia: data from St Vincent’s Hospital and associated screening clinics, Sydney, NSW. Clin Infect Dis. 2021;72(10):e649-e651. doi: 10.1093/cid/ciaa1256 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
