

REBOA for the Treatment of Blast Polytrauma: Zone 3 Provides Cerebral Perfusion, Attenuates Organ Dysfunction and Reperfusion Coagulopathy Compared to Zone 1 in a Swine Model
- PMID: 36749658
- PMCID: PMC10133017
- DOI: 10.1097/TA.0000000000003894
REBOA for the Treatment of Blast Polytrauma: Zone 3 Provides Cerebral Perfusion, Attenuates Organ Dysfunction and Reperfusion Coagulopathy Compared to Zone 1 in a Swine Model
Abstract
Background: Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a lifesaving therapy for hemorrhagic shock following pelvic/lower extremity injuries in military settings. However, Zone 1 aortic occlusion (AO; above the celiac artery), while providing brain/cardiac perfusion, may induce/worsen visceral ischemia and organ dysfunction. In contrast, AO Zone 3 (below the renal arteries) provides abdominal perfusion potentially minimizing ischemia/reperfusion injury. We hypothesized that, compared with AO Zone 1, AO Zone 3 provides neuro/cardioprotection while minimizing visceral ischemia and reperfusion coagulopathy after severe traumatic hemorrhage due to pelvic/lower extremity injuries.
Methods: Fifty-kilogram male Yorkshire swine underwent a blast polytrauma injury followed by a resuscitation protocol with randomization to no AO (No AO, n = 6) or AO with REBOA at Zone 1 (AO Zone 1; n = 6) or Zone 3 (AO Zone 3; n = 4). Vital signs and intracranial pressure (ICP) were monitored for 240 minutes. Citrate native and tissue plasminogen activator challenge thrombelastography, prothrombin time, creatinine, lipase, total bilirubin, troponin, and enzyme-linked immunosorbent assays protein levels were measured at set intervals.
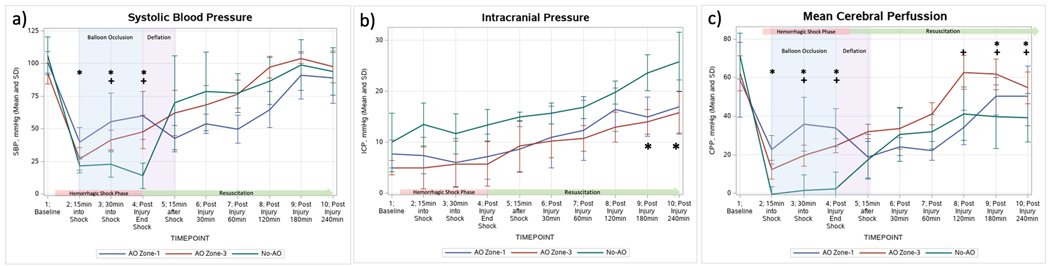
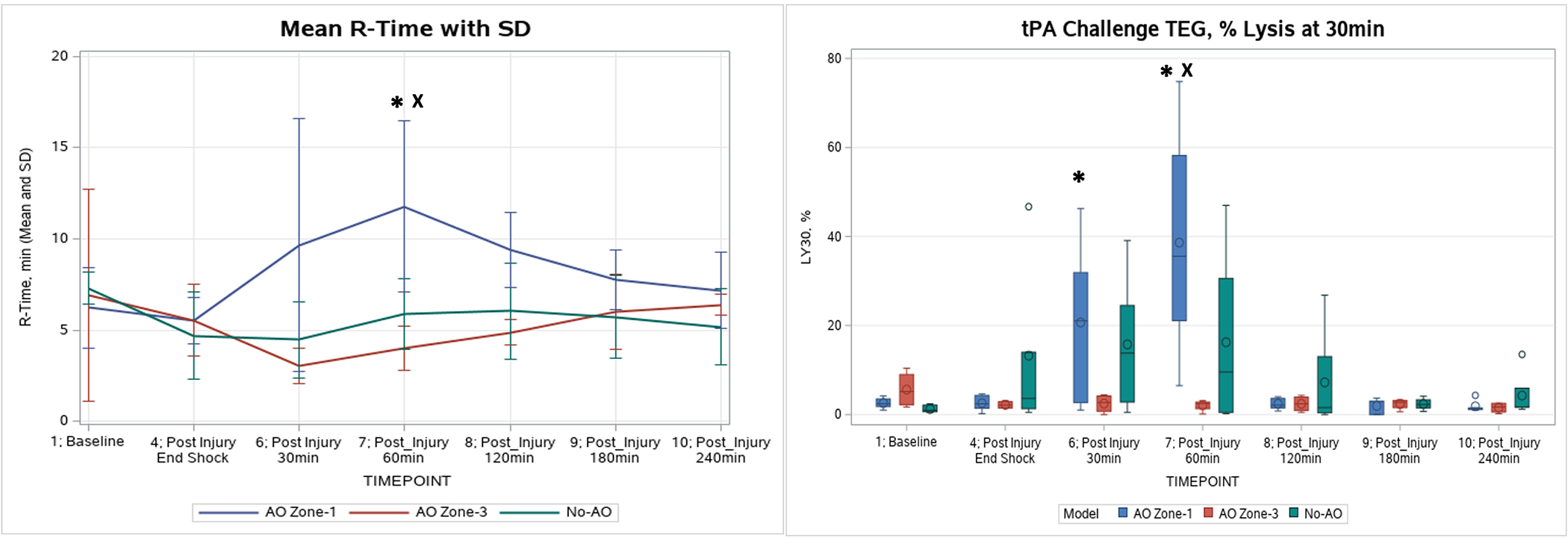
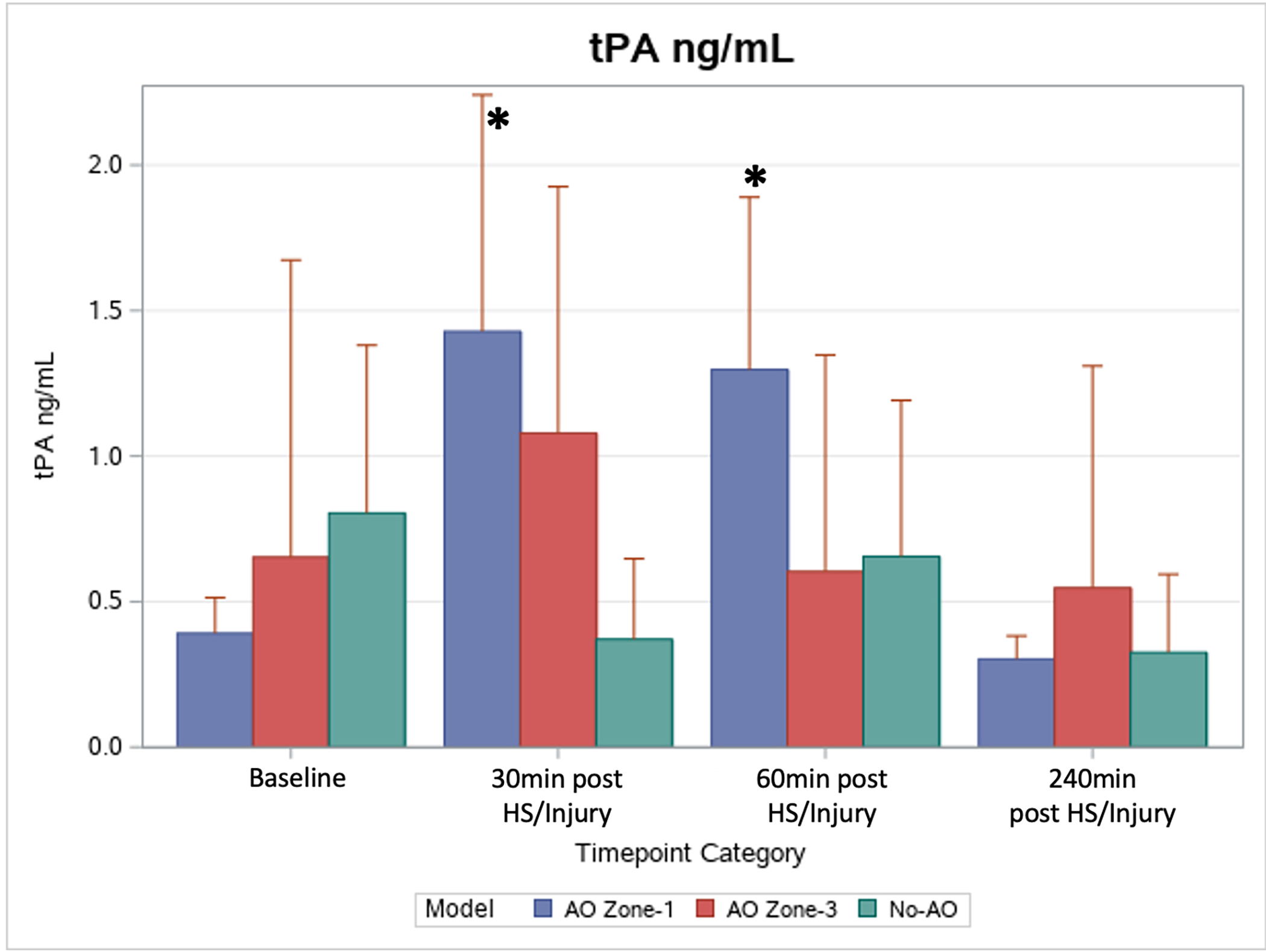
Results: Both AO groups had significant increases in mean arterial pressure during aortic occlusion. All three groups had significant increases in ICP, but final ICP in the No AO group (26 ± 5.8 mm Hg) was significantly elevated compared with AO Zone 1 (17 ± 5.2 mm Hg) and AO Zone 3 (16 ± 4.2 mm Hg) ( p < 0.01). The final mean troponin in the No AO group (4.10 ± 5.67 ng/mL) was significantly higher than baseline (0.03 ± 0.02 ng/mL, p < 0.05), while the two AO groups had no significant changes ( p > 0.05). AO Zone 1 was the only group associated with hyperfibrinolysis ( p < 0.05) and significantly increased prothrombin time ( p < 0.05). Only AO Zone 1 group had significantly higher markers of organ damage.
Conclusion: Compared with AO Zone 1, AO Zone 3 provided similar neuro/cardioprotection but with less organ dysfunction and coagulopathy. This study suggests that Zone 3 REBOA may be preferable over Zone 1 for treating military relevant blast polytrauma with minimal intra-abdominal and chest trauma, but further clinical investigation is warranted.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Cannon JW, Hofmann LJ, Glasgow SC, Potter BK, Rodriguez CJ, Cancio LC, et al. Dismounted Complex Blast Injuries: A Comprehensive Review of the Modern Combat Experience. J Am Coll Surg. 2016;223(4):652–64 e8. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, et al. Death on the battlefield (2001–2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S431–7. - PubMed
-
- Rasmussen TE, Eliason JL. Military-civilian partnership in device innovation: Development, commercialization and application of resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2017;83(4):732–5. - PubMed
-
- Northern DM, Manley JD, Lyon R, Farber D, Mitchell BJ, Filak KJ, et al. Recent advances in austere combat surgery: Use of aortic balloon occlusion as well as blood challenges by special operations medical forces in recent combat operations. J Trauma Acute Care Surg. 2018;85(1S Suppl 2):S98–S103. - PubMed
-
- Glaser J, Stigall K, Jensen CS, Morrison UJJ, Snyder S, & Russo MR. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) for Hemorrhagic Shock (CPG ID:38) JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE (JTS CPG). 31 Mar 2020:1–28.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
