

Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis
- PMID: 36750248
- PMCID: PMC9911127
- DOI: 10.9778/cmajo.20210119
Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis
Abstract
Background: Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.
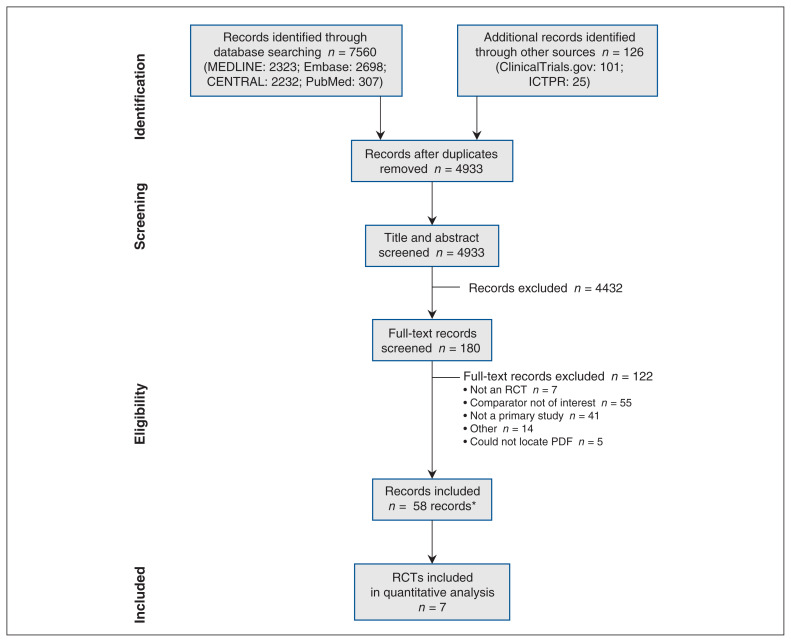
Methods: We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.
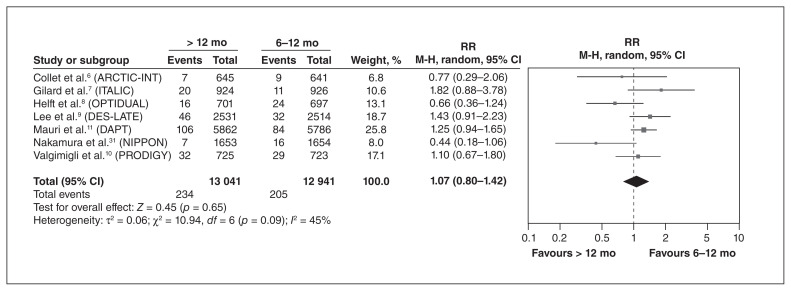
Results: We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.
Interpretation: Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.
Study registration: PROSPERO no. CRD42018082587.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Derek So has received unrestricted grants from Eli Lilly Canada and Spartan Biosciences for physician-initiated studies and has served as an advisory board member for AstraZeneca Canada. No other competing interests were declared.
Figures
Similar articles
-
Dual antiplatelet therapy following percutaneous coronary intervention: protocol for a systematic review.BMJ Open. 2019 Jun 16;9(6):e022271. doi: 10.1136/bmjopen-2018-022271. BMJ Open. 2019. PMID: 31209080 Free PMC article.
-
Three versus 12-month dual antiplatelet therapy duration in patients with acute coronary syndrome undergoing percutaneous coronary intervention: A meta-analysis of randomized controlled trials.Catheter Cardiovasc Interv. 2022 Dec;100(7):1151-1158. doi: 10.1002/ccd.30467. Epub 2022 Nov 3. Catheter Cardiovasc Interv. 2022. PMID: 36326115
-
Abbreviated ticagrelor based dual antiplatelet therapy in acute coronary syndrome: A systematic review and meta-analysis.Cardiovasc Revasc Med. 2025 Jun;75:64-70. doi: 10.1016/j.carrev.2024.09.005. Epub 2024 Sep 19. Cardiovasc Revasc Med. 2025. PMID: 39327142
-
Efficacy and safety of short-term dual antiplatelet therapy (≤6 months) after percutaneous coronary intervention for acute coronary syndrome: A systematic review and meta-analysis of randomized controlled trials.Clin Cardiol. 2018 Nov;41(11):1455-1462. doi: 10.1002/clc.23075. Epub 2018 Nov 20. Clin Cardiol. 2018. PMID: 30225978 Free PMC article.
-
The optimal discontinuation of dual antiplatelet therapy in patients undergoing percutaneous coronary intervention with drug-eluting stents: A meta-analysis of randomized trials.Int J Cardiol. 2017 May 15;235:73-86. doi: 10.1016/j.ijcard.2017.02.091. Epub 2017 Feb 24. Int J Cardiol. 2017. PMID: 28284499
Cited by
-
Patient-Related Factors Predicting Stent Thrombosis in Percutaneous Coronary Interventions.J Clin Med. 2023 Nov 28;12(23):7367. doi: 10.3390/jcm12237367. J Clin Med. 2023. PMID: 38068419 Free PMC article. Review.
-
Cangrelor - Expanding therapeutic options in patients with acute coronary syndrome.Cardiol J. 2024;31(1):133-146. doi: 10.5603/cj.96076. Epub 2023 Nov 15. Cardiol J. 2024. PMID: 37964649 Free PMC article.
References
-
- Elliott J, Kelly SE, Bai Z, et al. Optimal duration of dual antiplatelet therapy following percutaneous coronary intervention: an umbrella review. Can J Cardiol. 2019;35:1039–46. - PubMed
-
- Wells GA, Elliott J, Kelly S, et al. CADTH technology review. 8. Ottawa: Canadian Agency for Drugs and Technologies in Health (CADTH); 2017. Dual antiplatelet therapy following percutaneous coronary intervention: a review of the clinical impact of treatment duration. - PubMed
-
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines — an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guideline for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction, 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery [published erratum in Circulation 2016;134:e192–4] Circulation. 2016;134:e123–55. - PubMed
-
- Jeppsson A, Petricevic M, Kolh P, et al. 2017 European Society of Cardiology (ESC) focused update on dual antiplatelet therapy in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) Eur J Cardiothorac Surg. 2018;53:3–4. - PubMed
-
- Mehta SR, Bainey KR, Cantor WJ, et al. 2018 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology focused update of the guidelines for the use of antiplatelet therapy. Can J Cardiol. 2018;34:214–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous