

Levosimendan in patients undergoing extracorporeal membrane oxygenation after cardiac surgery: an emulated target trial using observational data
- PMID: 36750852
- PMCID: PMC9906922
- DOI: 10.1186/s13054-023-04328-6
Levosimendan in patients undergoing extracorporeal membrane oxygenation after cardiac surgery: an emulated target trial using observational data
Abstract
Background: Retrospective cohorts have suggested that levosimendan may facilitate the weaning of veno-arterial extracorporeal membrane oxygenation (VA-ECMO). We therefore studied this clinical question by emulating a randomized trial with observational data.
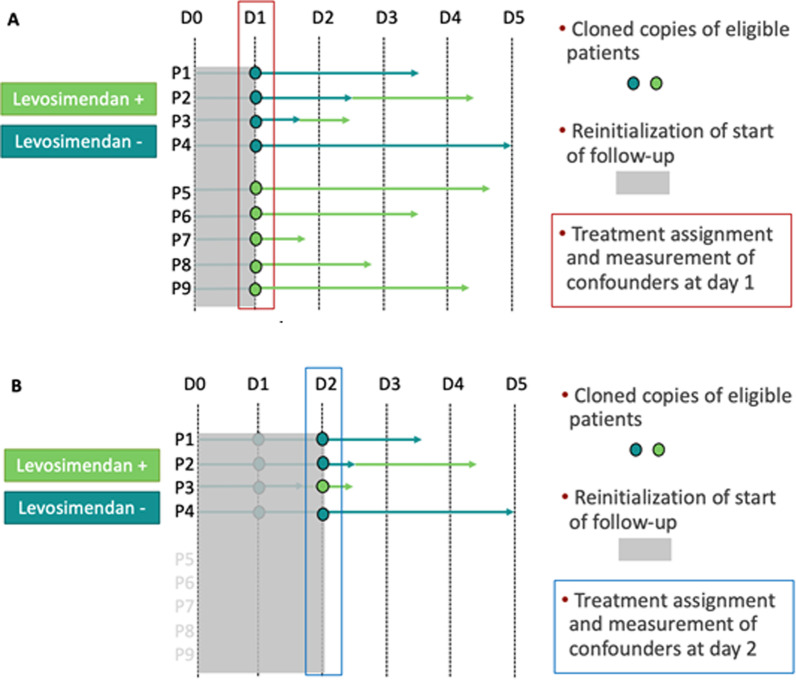
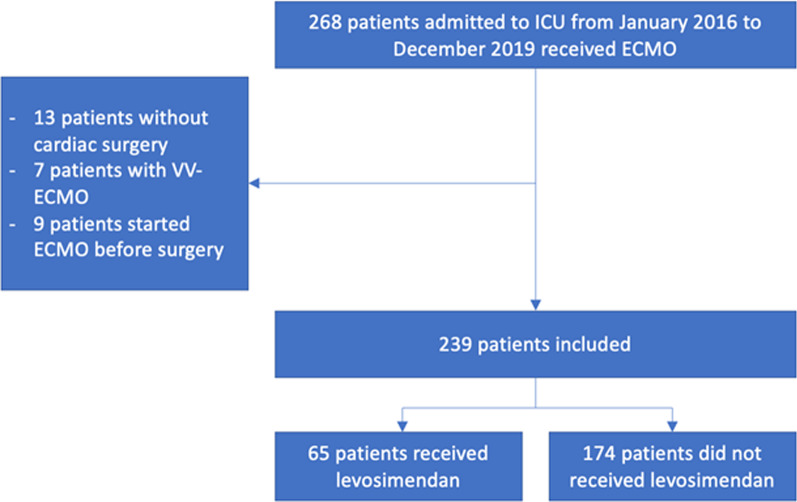
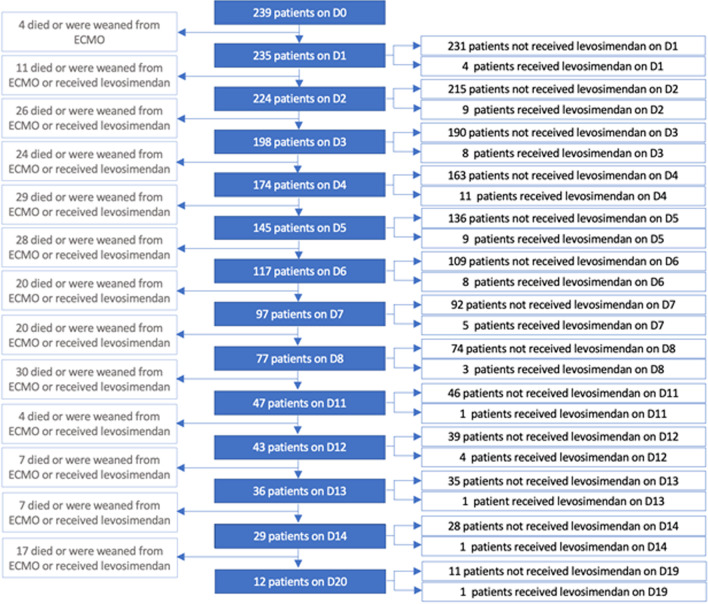
Methods: All patients with refractory postcardiotomy cardiogenic shock and assisted with VA-ECMO, admitted to a surgical intensive care unit at La Pitié-Salpêtrière Hospital between 2016 and 2019, were eligible. To avoid immortal-time bias, we emulated a target trial sequentially comparing levosimendan administration versus no levosimendan administration in patients treated with VA-ECMO. The primary outcome was time to successful ECMO weaning. The secondary outcomes were 30-day and 1-year mortality. We performed a multivariable analysis to adjust for confounding at baseline.
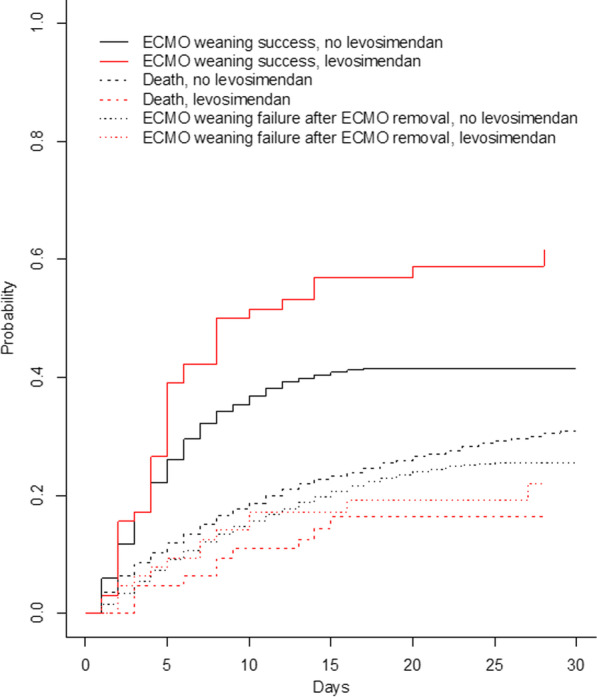
Results: Two hundred and thirty-nine patients were included in the study allowing building a nested trials cohort of 1434 copies of patients. No association of levosimendan treatment and VA-ECMO weaning was found (HR = 0.91, [0.57; 1.45], p = 0.659 in multivariable analysis), or 30-day mortality (OR = 1.03, [0.52; 2.03], p = 0.940) and 1-year mortality (OR = 1.00, [0.53; 1.89], p = 0.999).
Conclusions: Using the emulated target trial framework, this study did not find any association of levosimendan treatment and ECMO weaning success after postcardiotomy cardiogenic shock. However, the population of interest remains heterogeneous and subgroups might benefit from levosimendan.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Can levosimendan reduce ECMO weaning failure in cardiogenic shock?: a cohort study with propensity score analysis.Crit Care. 2020 Jul 16;24(1):442. doi: 10.1186/s13054-020-03122-y. Crit Care. 2020. PMID: 32677985 Free PMC article.
-
Short-term effects of levosimendan use for venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis.Perfusion. 2023 Mar;38(2):305-312. doi: 10.1177/02676591211051860. Epub 2021 Oct 23. Perfusion. 2023. PMID: 34689640
-
Effects of levosimendan on weaning and survival in adult cardiogenic shock patients with veno-arterial extracorporeal membrane oxygenation: systematic review and meta-analysis.Perfusion. 2020 Sep;35(6):484-491. doi: 10.1177/0267659120918473. Epub 2020 May 24. Perfusion. 2020. PMID: 32449494
-
Role of levosimendan in weaning children requiring veno-arterial extracorporeal membrane oxygenation after cardiac surgery.Eur J Cardiothorac Surg. 2021 Jan 4;59(1):262-268. doi: 10.1093/ejcts/ezaa275. Eur J Cardiothorac Surg. 2021. PMID: 32910173
-
Beneficial effects of levosimendan to wean patients from VA-ECMO: a systematic review and meta-analysis.Minerva Cardiol Angiol. 2023 Oct;71(5):564-574. doi: 10.23736/S2724-5683.22.06054-9. Epub 2022 Jun 10. Minerva Cardiol Angiol. 2023. PMID: 35687316
Cited by
-
Near-infrared spectroscopy and ultrasound as complementary methods for assessing organ and peripheral tissue perfusion in veno-arterial-ECMO patients.Am J Transl Res. 2025 Apr 15;17(4):2629-2641. doi: 10.62347/UQYS8766. eCollection 2025. Am J Transl Res. 2025. PMID: 40385015 Free PMC article.
-
Unlocking the Therapeutic Symphony: A Systematic Review Exploring the Role of Levosimendan in the Management of Heart Failure.Cureus. 2024 Jun 20;16(6):e62799. doi: 10.7759/cureus.62799. eCollection 2024 Jun. Cureus. 2024. PMID: 39036117 Free PMC article. Review.
-
Does Levosimendan hasten veno-arterial ECMO weaning? A propensity score matching analysis.Ann Intensive Care. 2025 Apr 3;15(1):48. doi: 10.1186/s13613-025-01457-9. Ann Intensive Care. 2025. PMID: 40180673 Free PMC article.
-
Use of vasopressors and inotropes in ECMO.Intensive Care Med. 2024 Mar;50(3):463-466. doi: 10.1007/s00134-024-07338-2. Epub 2024 Feb 19. Intensive Care Med. 2024. PMID: 38372746 No abstract available.
-
Methodologies for the Emulation of Biomarker-Guided Trials Using Observational Data: A Systematic Review.J Pers Med. 2025 May 10;15(5):195. doi: 10.3390/jpm15050195. J Pers Med. 2025. PMID: 40423066 Free PMC article. Review.
References
-
- Lorusso R, Raffa GM, Alenizy K, Sluijpers N, Makhoul M, Brodie D, et al. Structured review of post-cardiotomy extracorporeal membrane oxygenation: part 1-Adult patients. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. 2019;38:1125–1143. doi: 10.1016/j.healun.2019.08.014. - DOI - PMC - PubMed
-
- Baran DA, Grines CL, Bailey S, Burkhoff D, Hall SA, Henry TD, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter Cardiovasc Interv Off J Soc Card Angiogr Interv. 2019;94:29–37. doi: 10.1002/ccd.28329. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
