

Endoscopic hematoma evacuation for acute subdural hematoma with improvement of the visibility of the subdural space and postoperative management using an intracranial pressure sensor
- PMID: 36751441
- PMCID: PMC9899456
- DOI: 10.25259/SNI_1084_2022
Endoscopic hematoma evacuation for acute subdural hematoma with improvement of the visibility of the subdural space and postoperative management using an intracranial pressure sensor
Abstract
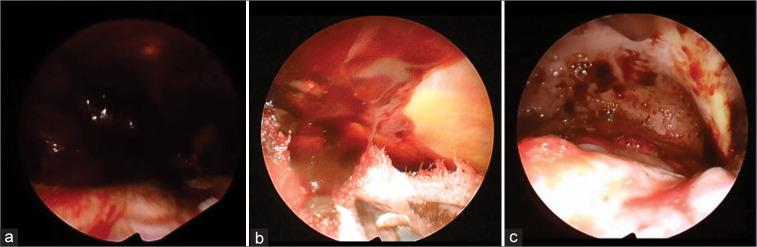
Background: The first choice to treat acute subdural hematoma (ASDH) is large craniotomy under general anesthesia. However, increasing age or the comorbid burden of patients may render invasive treatment strategy inappropriate. These medically frail patients with ASDH may benefit from a combination of small craniotomy and endoscopic hematoma removal, which is less invasive. We proposed covering with protective sheets to prevent brain injury due to contact with the endoscope and suction cannula and improve visualization of the subdural space. Moreover, we placed an intracranial pressure (ICP) sensor after endoscopic hematoma removal. In this article, we attempted to clarify the use of small craniotomy evacuation with endoscopy for ASDH.
Methods: Between January 2015 and December 2019, nine patients with ASDH underwent hematoma evacuation with endoscopy at our hospital. ASDH was removed using a suction tube with the aid of a rigid endoscope through the small craniotomy (5-6 cm). Improvement of the clinical symptoms and procedure-related complications was evaluated.
Results: No procedure-related hemorrhagic complications were observed. The outcomes of our endoscopic surgery were satisfactory without complications or rebleeding. The outcomes were not inferior to those of other reported endoscopic surgeries.
Conclusion: The results suggest that small craniotomy evacuation with endoscopy and postoperative management using an ICP sensor is a safe, effective, and minimally invasive treatment approach for ASDH in appropriately selected cases.
Keywords: Acute subdural hematoma; Endoscopic hematoma evacuation; Intracranial pressure; Minimally invasive; Small craniotomy; Surgical technique; Traumatic brain injury.
Copyright: © 2023 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures



References
-
- Codd PJ, Venteicher AS, Agarwalla PK, Kahle KT, Jho DH. Endoscopic burr hole evacuation of an acute subdural hematoma. J Clin Neurosci. 2013;20:1751–3. - PubMed
-
- Hwang SC, Shin DS. Endoscopic treatment of acute subdural hematoma with a normal small craniotomy. J Neurol Surg A Cent Eur Neurosurg. 2020;81:10–6. - PubMed
-
- Ichimura S, Takahara K, Nakaya M, Yoshida K, Mochizuki Y, Fukuchi M, et al. Neuroendoscopic hematoma removal with a small craniotomy for acute subdural hematoma. J Clin Neurosci. 2019;61:311–4. - PubMed
-
- Katsuki M, Kakizawa Y, Nishikawa A, Kunitoki K, Yamamoto Y, Wada N, et al. Fifteen cases of endoscopic treatment of acute subdural hematoma with small craniotomy under local anesthesia: Endoscopic hematoma removal reduces the intraoperative bleeding amount and the operative time compared with craniotomy in patients aged 70 or older. Neurol Med Chir. 2020;60:439–49. - PMC - PubMed
-
- Kawasaki T, Kurosaki Y, Fukuda H, Kinosada M, Ishibashi R, Handa A, et al. Flexible endoscopically assisted evacuation of acute and subacute subdural hematoma through a small craniotomy: Preliminary results. Acta Neurochir. 2018;160:241–8. - PubMed
LinkOut - more resources
Full Text Sources