

Design and development of a digital shared decision-making tool for stroke prevention in atrial fibrillation
- PMID: 36751465
- PMCID: PMC9893868
- DOI: 10.1093/jamiaopen/ooad003
Design and development of a digital shared decision-making tool for stroke prevention in atrial fibrillation
Abstract
Background: Shared decision-making (SDM) is an approach in which patients and clinicians act as partners in making medical decisions. Patients receive the information needed to decide and are encouraged to balance risks, benefits, and preferences. Informative materials are vital to SDM. Atrial fibrillation (AF) is the most common cardiac arrhythmia and responsible for 10% of ischemic strokes, however 1/3 of patients are not on appropriate anticoagulation. Decision sharing may facilitate treatment acceptance, improving outcomes.
Aims: To develop a framework of the components needed to create novel SDM tools and to provide practical examples through a case-study of stroke prevention in AF.
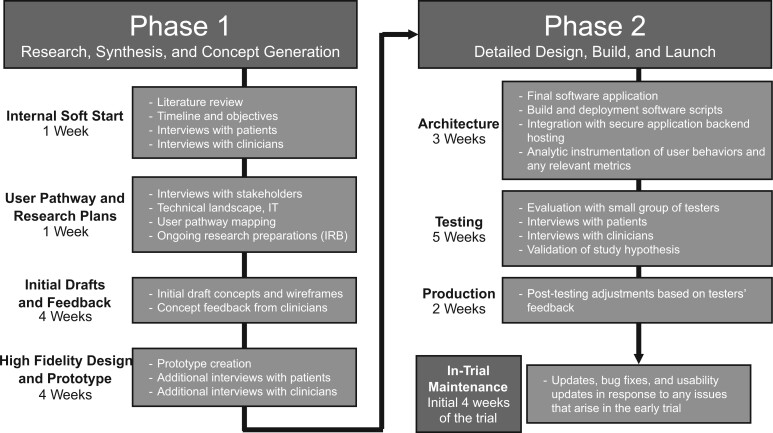
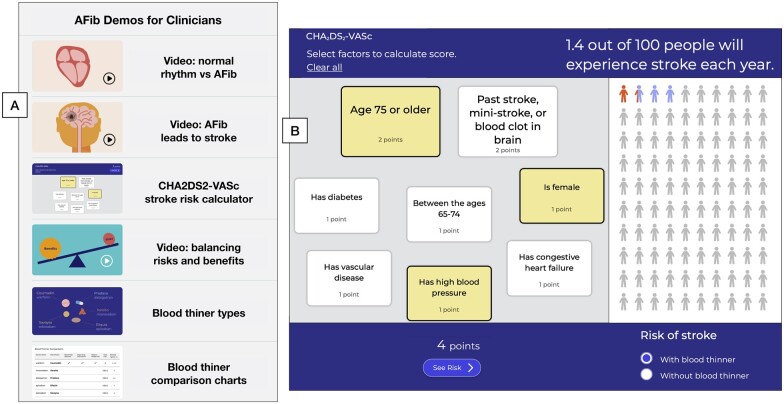
Methods: We analyze the design values of a web-based SDM tool created to better inform AF patients about anticoagulation. The tool was developed in partnership with patient advocates, multi-disciplinary investigators, and private design firms. It was refined through iterative, recursive testing in patients with AF. Its effectiveness is being evaluated in a multisite clinical trial led by Stanford University and sponsored by the American Heart Association.
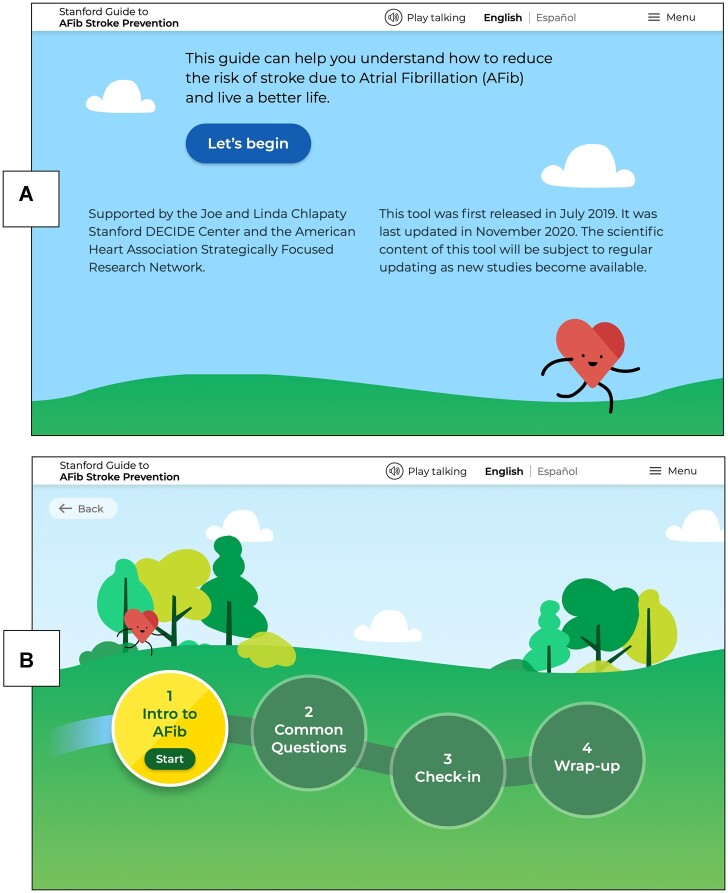
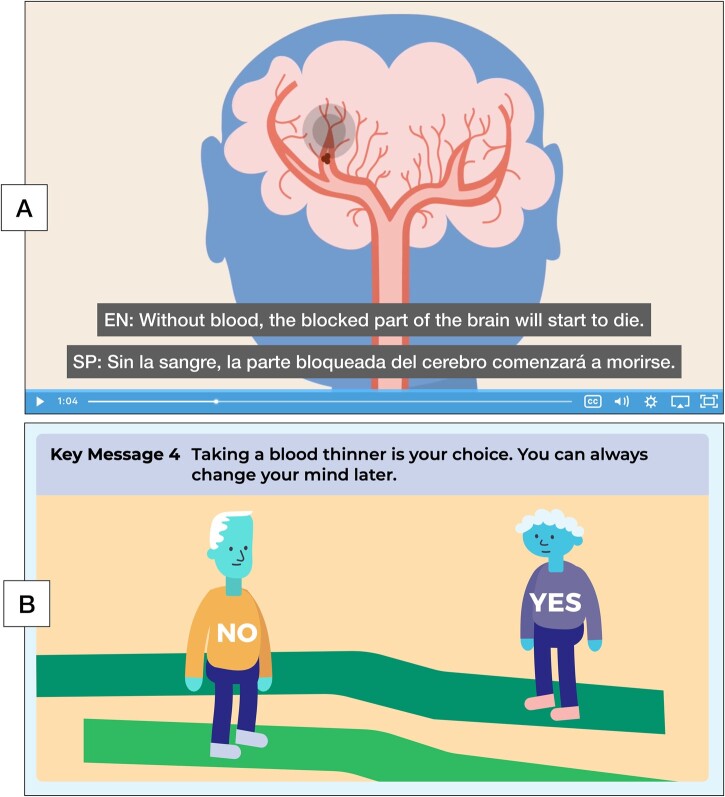
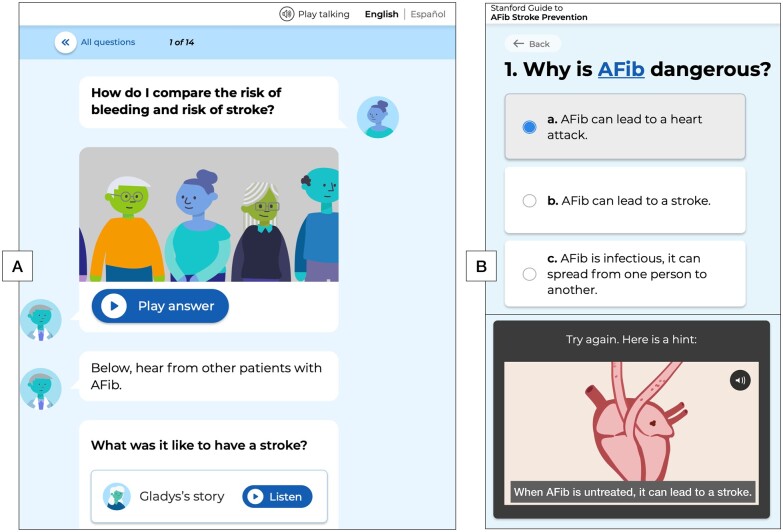
Findings: The main components considered when creating the Stanford AFib tool included: design and software; content identification; information delivery; inclusive communication, user engagement; patient feedback; clinician experience; and anticipation of implementation and dissemination. We also highlight the ethical principles underlying SDM; matters of diversity and inclusion, linguistic variety, accessibility, and health literacy. The Stanford AFib Guide patient tool is available at: https://afibguide.com and the clinician tool at https://afibguide.com/clinician.
Conclusion: Attention to a range of vital development and design factors can facilitate tool adoption and information acquisition by diverse cultural, educational, and socioeconomic subpopulations. With thoughtful design, digital tools may decrease decision regret and improve treatment outcomes across many decision-making situations in healthcare.
Keywords: atrial fibrillation; medical design; patient decision aid; research tools; shared decision-making.
© The Author(s) 2023. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Figures
Similar articles
-
The ENHANCE-AF clinical trial to evaluate an atrial fibrillation shared decision-making pathway: Rationale and study design.Am Heart J. 2022 May;247:68-75. doi: 10.1016/j.ahj.2022.01.013. Epub 2022 Jan 28. Am Heart J. 2022. PMID: 35092723 Clinical Trial.
-
Development of a shared decision-making tool to assist patients and clinicians with decisions on oral anticoagulant treatment for atrial fibrillation.Curr Med Res Opin. 2015 Dec;31(12):2261-72. doi: 10.1185/03007995.2015.1096767. Epub 2015 Oct 22. Curr Med Res Opin. 2015. PMID: 26390360
-
Development of Complementary Encounter and Patient Decision Aids for Shared Decision Making about Stroke Prevention in Atrial Fibrillation.MDM Policy Pract. 2023 Jun 21;8(1):23814683231178033. doi: 10.1177/23814683231178033. eCollection 2023 Jan-Jun. MDM Policy Pract. 2023. PMID: 38178866 Free PMC article.
-
Shared Decision Making Tools for People Facing Stroke Prevention Strategies in Atrial Fibrillation: A Systematic Review and Environmental Scan.Med Decis Making. 2021 Jul;41(5):540-549. doi: 10.1177/0272989X211005655. Epub 2021 Apr 24. Med Decis Making. 2021. PMID: 33896270 Free PMC article.
-
Decision aids for shared decision-making and appropriate anticoagulation therapy in patients with atrial fibrillation: a systematic review and meta-analysis.Eur J Cardiovasc Nurs. 2022 Mar 3;21(2):97-106. doi: 10.1093/eurjcn/zvab085. Eur J Cardiovasc Nurs. 2022. PMID: 34550376
Cited by
-
Development of web- and mobile-based shared decision-making tools in the neurological intensive care unit.Neurotherapeutics. 2025 Jan;22(1):e00503. doi: 10.1016/j.neurot.2024.e00503. Epub 2024 Dec 6. Neurotherapeutics. 2025. PMID: 39643583 Free PMC article. Review.
-
Patient-Selection of a Clinical Trial Primary Outcome: The ENHANCE-AF Outcomes Survey.PLoS One. 2025 Mar 7;20(3):e0318858. doi: 10.1371/journal.pone.0318858. eCollection 2025. PLoS One. 2025. PMID: 40053524 Free PMC article.
References
-
- O’Connor AM, Wennberg JE, Legare F, et al.Toward the “tipping point”: decision aids and informed patient choice. Health Aff (Millwood) 2007; 26 (3): 716–25. - PubMed
-
- Emanuel EJ, Emanuel LL.. Four models of the physician-patient relationship. JAMA 1992; 267 (16): 2221–6. - PubMed
-
- Elwyn G, Coulter A, Laitner S, Walker E, Watson P, Thomson R.. Implementing shared decision making in the NHS. BMJ 2010; 341: c5146. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical