

Mobile SARS‑CoV‑2 screening facilities for rapid deployment and university-based diagnostic laboratory
- PMID: 36751470
- PMCID: PMC9893752
- DOI: 10.1002/elsc.202200026
Mobile SARS‑CoV‑2 screening facilities for rapid deployment and university-based diagnostic laboratory
Abstract
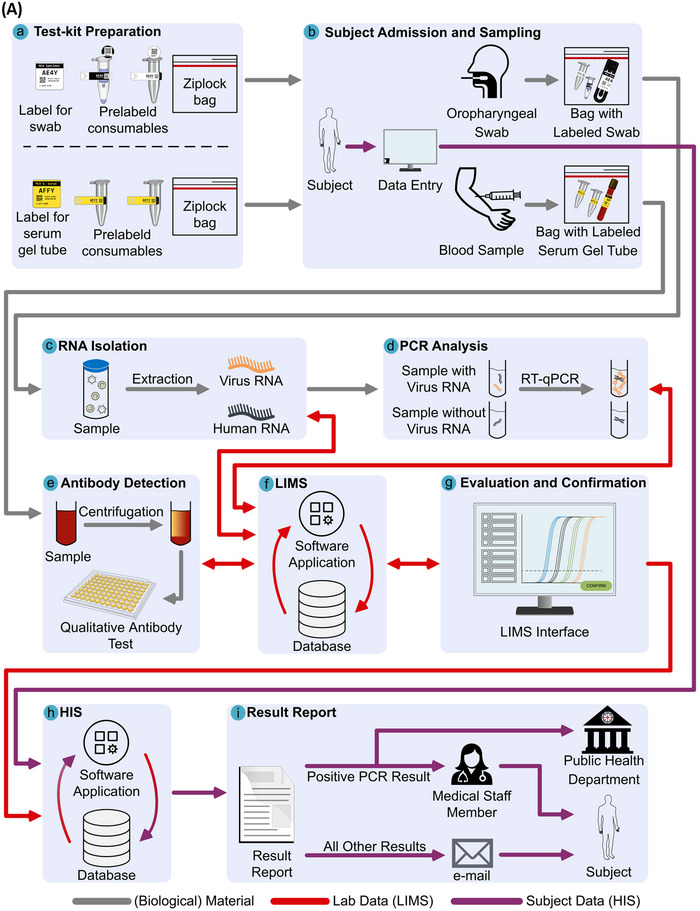
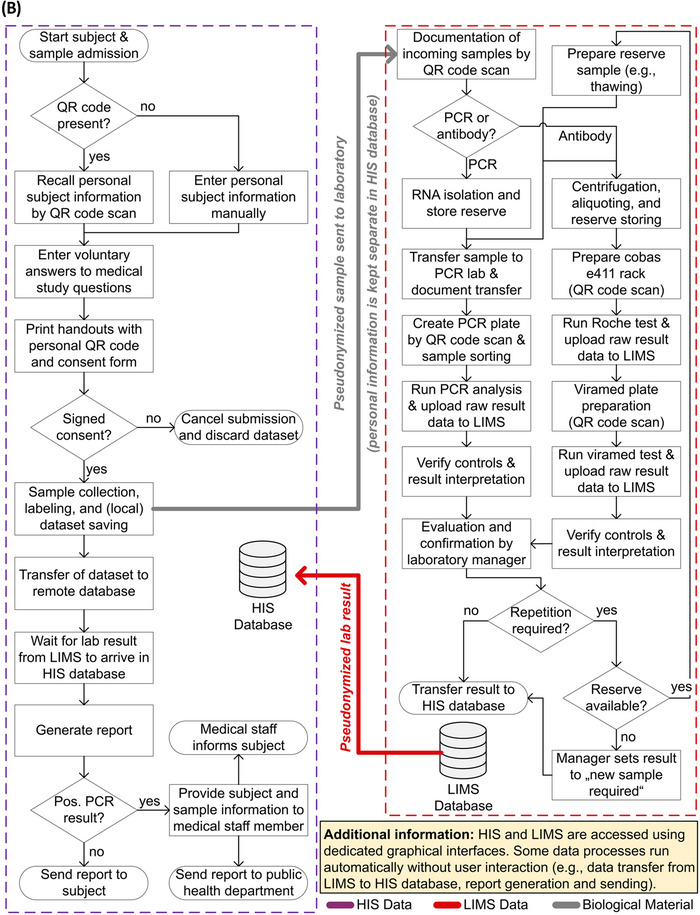
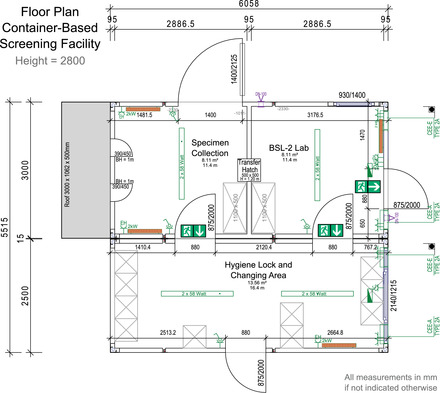
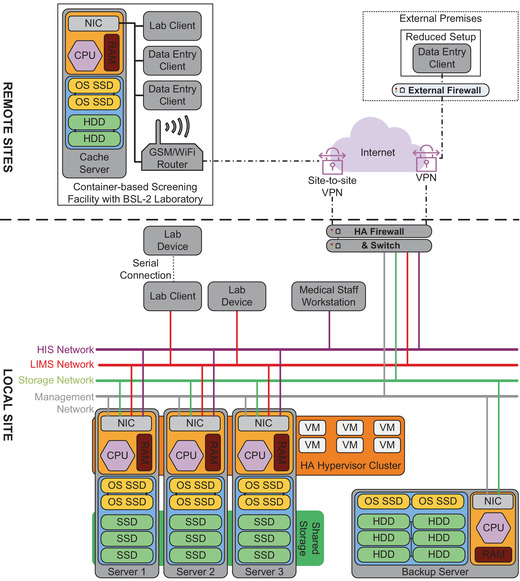
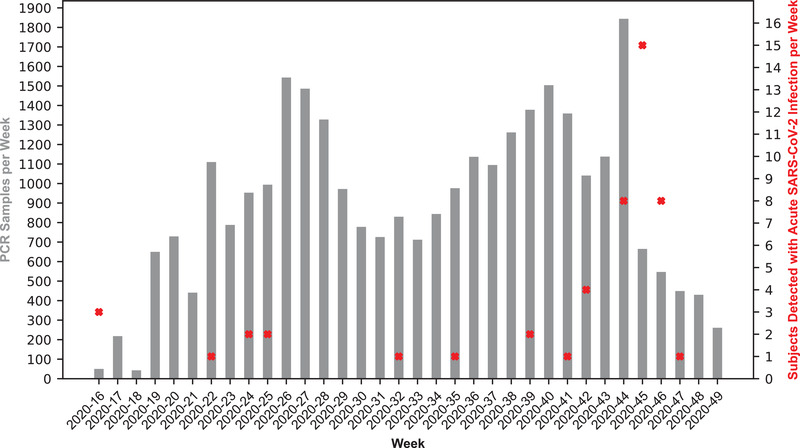
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has created a public crisis. Many medical and public institutions and businesses went into isolation in response to the pandemic. Because SARS-CoV-2 can spread irrespective of a patient's course of disease, these institutions' continued operation or reopening based on the assessment and control of virus spread can be supported by targeted population screening. For this purpose, virus testing in the form of polymerase chain reaction (PCR) analysis and antibody detection in blood can be central. Mobile SARS-CoV-2 screening facilities with a built-in biosafety level (BSL)-2 laboratory were set up to allow the testing offer to be brought close to the subject group's workplace. University staff members, their expertise, and already available equipment were used to implement and operate the screening facilities and a certified diagnostic laboratory. This operation also included specimen collection, transport, PCR and antibody analysis, and informing subjects as well as public health departments. Screening facilities were established at different locations such as educational institutions, nursing homes, and companies providing critical supply chains for health care. Less than 4 weeks after the first imposed lockdown in Germany, a first mobile testing station was established featuring a build-in laboratory with two similar stations commencing operation until June 2020. During the 15-month project period, approximately 33,000 PCR tests and close to 7000 antibody detection tests were collected and analyzed. The presented approach describes the required procedures that enabled the screening facilities and laboratories to collect and process several hundred specimens each day under difficult conditions. This report can assist others in establishing similar setups for pandemic scenarios.
Keywords: COVID‐19; HIS & LIMS; PCR; SARS‐CoV‐2; screening.
© 2023 The Authors. Engineering in Life Sciences published by Wiley‐VCH GmbH.
Conflict of interest statement
The authors have declared no conflicts of interest.
Figures

References
-
- Stanislawski N, Lange F, Fahnemann C, et al. MCA Dataset, LUIS, 2022. doi: 10.25835/jt0dobsz - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous