

Autoantibodies are highly prevalent in non-SARS-CoV-2 respiratory infections and critical illness
- PMID: 36752204
- PMCID: PMC9977421
- DOI: 10.1172/jci.insight.163150
Autoantibodies are highly prevalent in non-SARS-CoV-2 respiratory infections and critical illness
Abstract
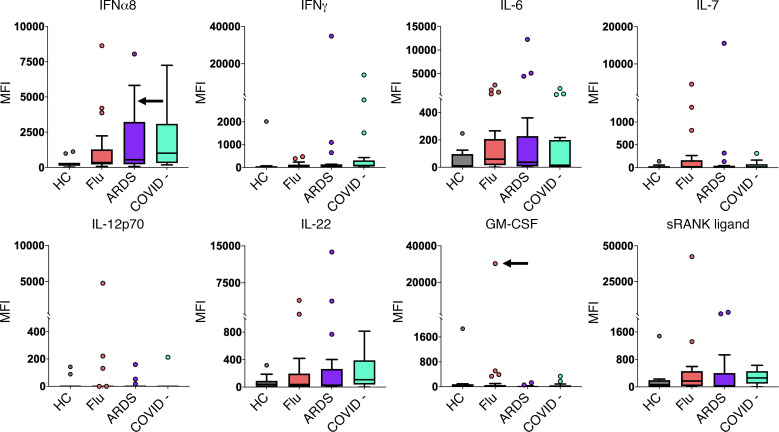
The widespread presence of autoantibodies in acute infection with SARS-CoV-2 is increasingly recognized, but the prevalence of autoantibodies in non-SARS-CoV-2 infections and critical illness has not yet been reported. We profiled IgG autoantibodies in 267 patients from 5 independent cohorts with non-SARS-CoV-2 viral, bacterial, and noninfectious critical illness. Serum samples were screened using Luminex arrays that included 58 cytokines and 55 autoantigens, many of which are associated with connective tissue diseases (CTDs). Samples positive for anti-cytokine antibodies were tested for receptor blocking activity using cell-based functional assays. Anti-cytokine antibodies were identified in > 50% of patients across all 5 acutely ill cohorts. In critically ill patients, anti-cytokine antibodies were far more common in infected versus uninfected patients. In cell-based functional assays, 11 of 39 samples positive for select anti-cytokine antibodies displayed receptor blocking activity against surface receptors for Type I IFN, GM-CSF, and IL-6. Autoantibodies against CTD-associated autoantigens were also commonly observed, including newly detected antibodies that emerged in longitudinal samples. These findings demonstrate that anti-cytokine and autoantibodies are common across different viral and nonviral infections and range in severity of illness.
Keywords: Adaptive immunity; Autoimmunity; Bacterial infections; Infectious disease; Influenza.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
