

Association of Long-term Change in N-Terminal Pro-B-Type Natriuretic Peptide With Incident Heart Failure and Death
- PMID: 36753229
- PMCID: PMC9909572
- DOI: 10.1001/jamacardio.2022.5309
Association of Long-term Change in N-Terminal Pro-B-Type Natriuretic Peptide With Incident Heart Failure and Death
Abstract
Importance: Most studies, especially in primary prevention patients, have evaluated N-terminal B-type natriuretic peptide (NT-proBNP) at one time point. Evaluation of change in NT-proBNP may improve risk stratification for incident cardiovascular events.
Objective: To assess the association between change in NT-proBNP and risk for incident heart failure (HF) and death.
Design, setting, and participants: Participants were recruited from 4 US communities enrolled in the Atherosclerosis Risk in Community (ARIC) study. Individuals who attended ARIC visits 2 and 4 (approximately 6 years apart) with measurements of NT-proBNP and without prevalent HF were included. Assays of NT-proBNP were conducted between 2011 and 2013, and analysis took place between July 2021 and October 2022.
Exposures: The primary exposure variable was NT-proBNP change between visits 2 and 4, modeled as change categories (<125 pg/mL or ≥125 pg/mL) and as percent change.
Main outcomes and measures: The primary outcome measures were incident HF hospitalization and all-cause death. The association between changes in cardiovascular risk factors with change in NT-proBNP was further assessed.
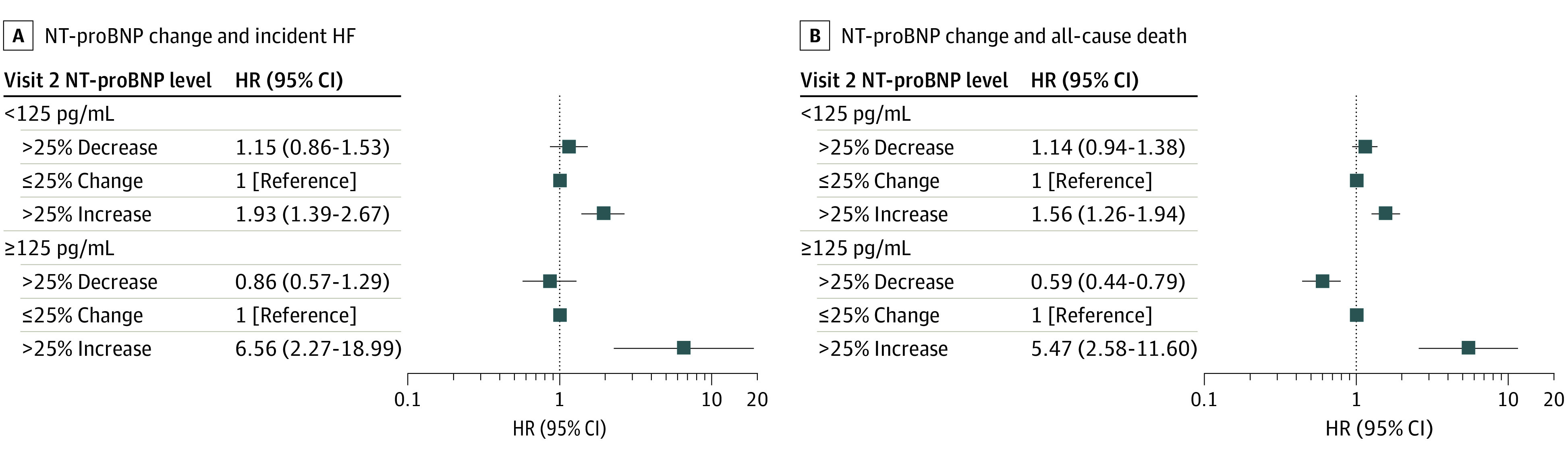
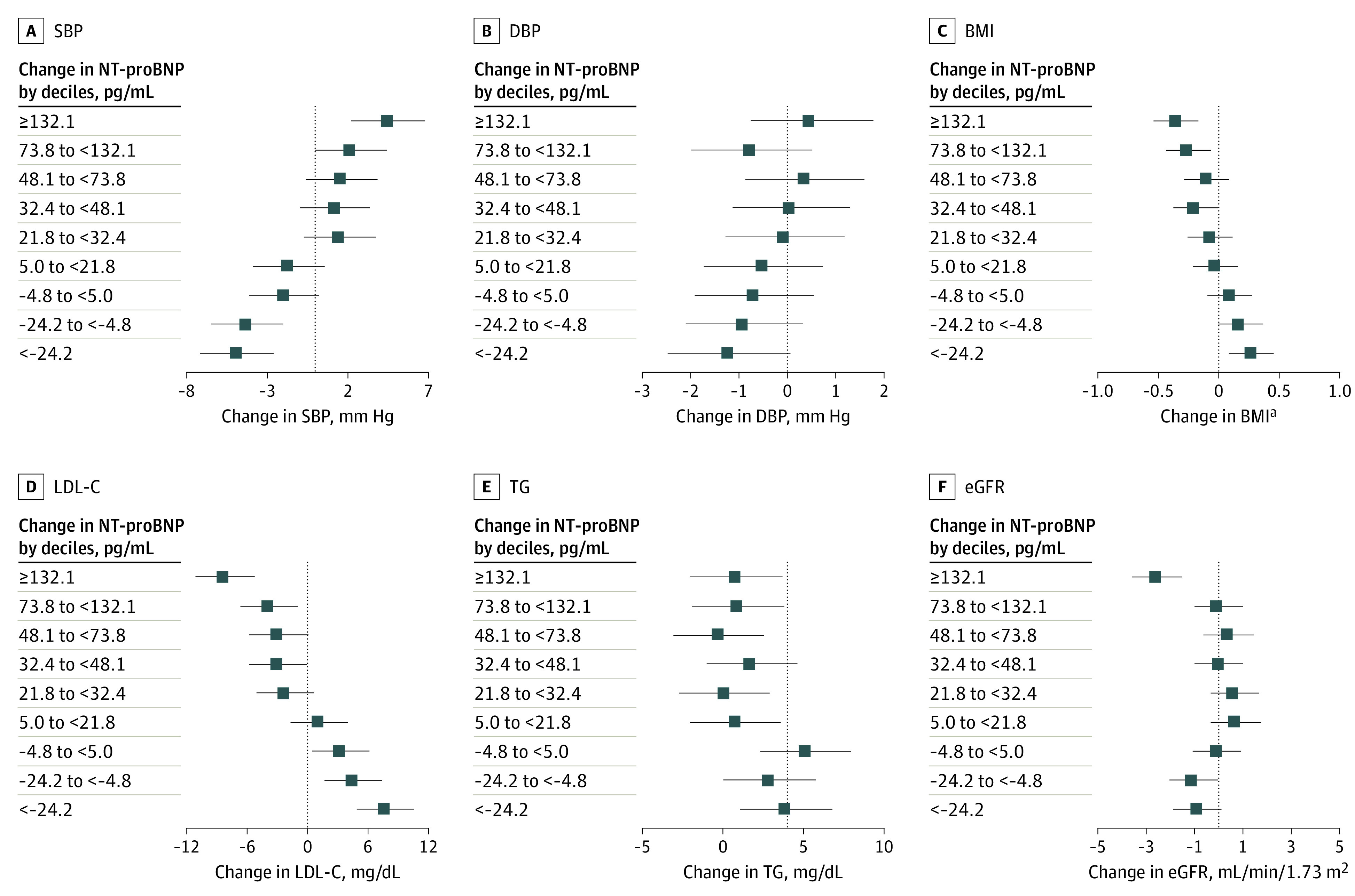
Results: A total of 9776 individuals (mean [SD] age, 57.1 [5.7] years at visit 2; 5523 [56.5%] women) were included in the study. Compared with participants with NT-proBNP level less than 125 pg/mL at both visits, participants with NT-proBNP level of 125 pg/mL or higher at both visits had an increase in incident HF (adjusted hazard ratio [HR], 2.40 [95% CI, 2.00-2.88]) and mortality risk (HR, 1.68 [95% CI, 1.47-1.91). Participants with NT-proBNP levels of 125 pg/mL or higher at visit 2 and less than 125 pg/mL at visit 4 had similar risk for HF and death (HR, 1.01 [95% CI, 0.71-1.43]; HR, 0.79 [95% CI, 0.61-1.01]) compared with the group with NT-proBNP levels of less than 125 pg/mL at both visits. The percent change in NT-proBNP was positively associated with HF and death (HR, 1.06 [95% CI, 1.02-1.10]; HR, 1.05 [95% CI, 1.03-1.08] per 1-SD increase, respectively). Change in systolic blood pressure, low-density lipoprotein cholesterol, triglyceride level, body mass index, and estimated glomerular filtration rate were significantly associated with change in NT-proBNP.
Conclusions and relevance: In this study, 6-year change in NT-proBNP reflected dynamic change in risk for HF events and death among community-dwelling adults without prevalent clinical HF. These results support the utility of serial NT-proBNP measurements to improve risk stratification of patients with pre-HF.
Conflict of interest statement
Figures
Comment in
-
Serial N-Terminal Pro-B-Type Natriuretic Peptide Measurements in the Population Without Clinical Heart Failure.JAMA Cardiol. 2023 Sep 1;8(9):889. doi: 10.1001/jamacardio.2023.1962. JAMA Cardiol. 2023. PMID: 37436731 No abstract available.
-
Serial N-Terminal Pro-B-Type Natriuretic Peptide Measurements in the Population Without Clinical Heart Failure-Reply.JAMA Cardiol. 2023 Sep 1;8(9):889-890. doi: 10.1001/jamacardio.2023.1965. JAMA Cardiol. 2023. PMID: 37436758 No abstract available.
References
-
- Wang TJ, Larson MG, Levy D, et al. . Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med. 2004;350(7):655-663. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, et al. . 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895-–e1032.. doi:10.1161/CIR.0000000000001063 - DOI - PubMed
-
- Bozkurt B, Coats AJ, Tsutsui H, et al. . Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J Card Fail. 2021;S1071-9164(21)00050-6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
