

Immunotoxin-αCD40 therapy activates innate and adaptive immunity and generates a durable antitumor response in glioblastoma models
- PMID: 36753564
- PMCID: PMC10440725
- DOI: 10.1126/scitranslmed.abn5649
Immunotoxin-αCD40 therapy activates innate and adaptive immunity and generates a durable antitumor response in glioblastoma models
Abstract
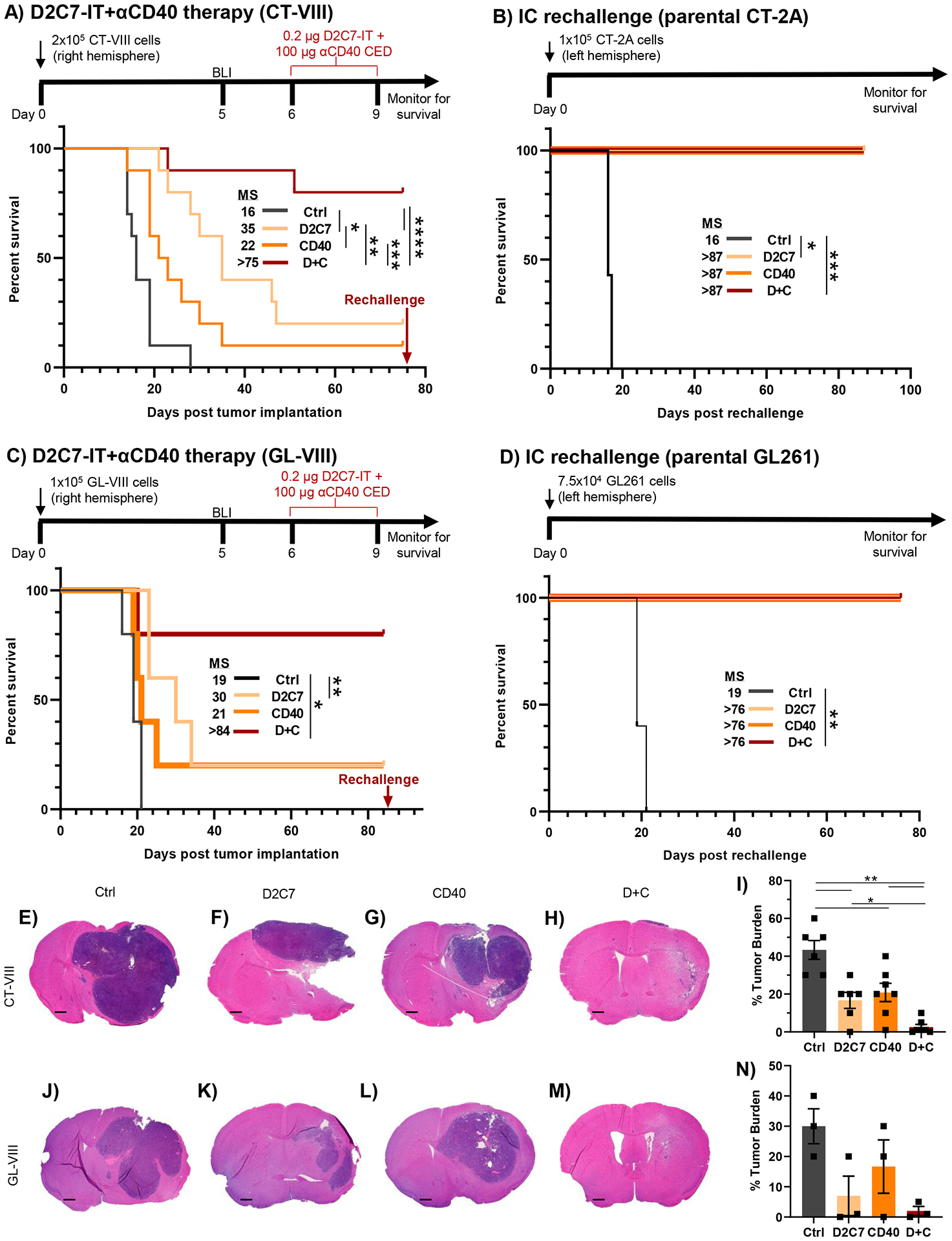
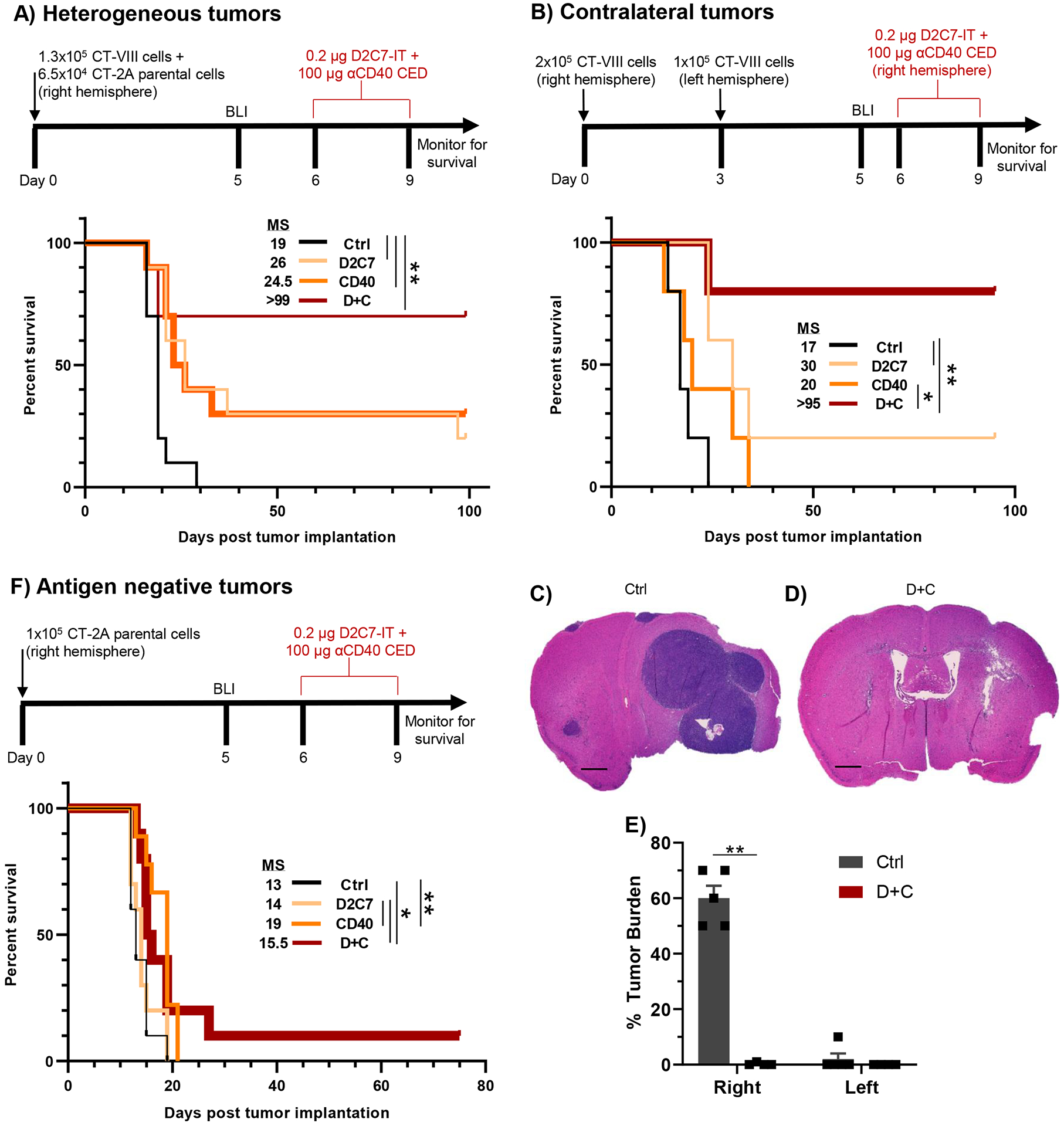
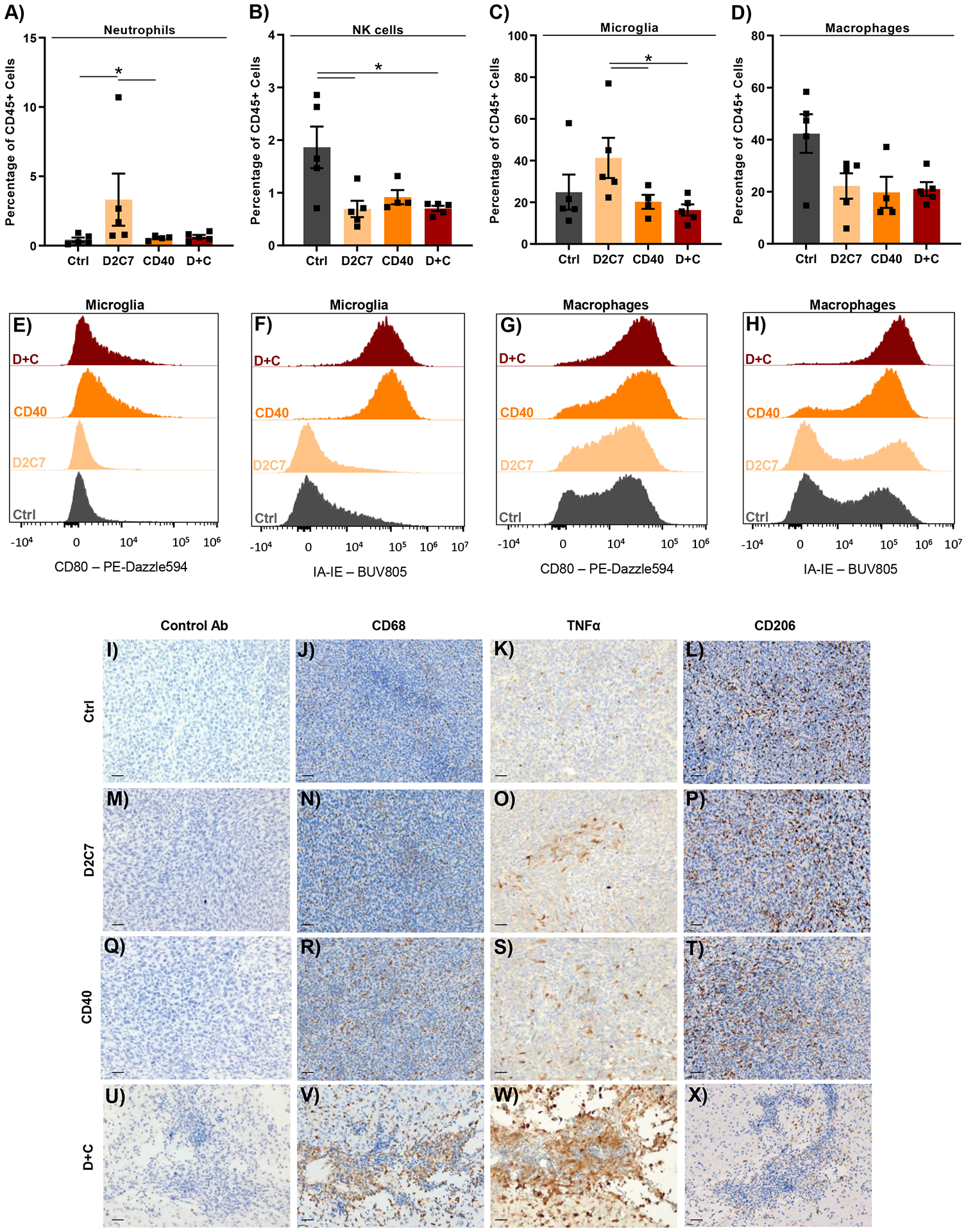
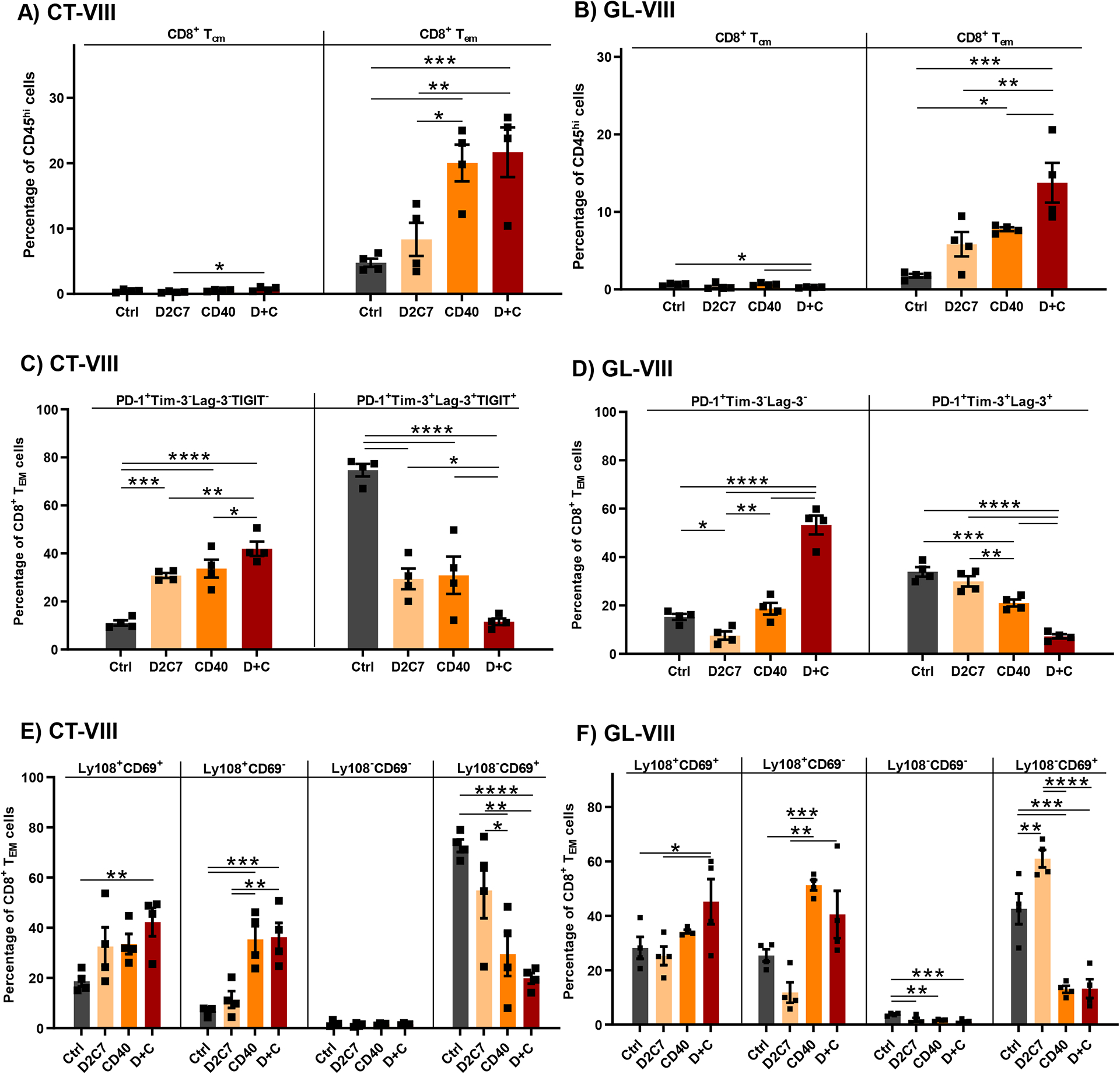
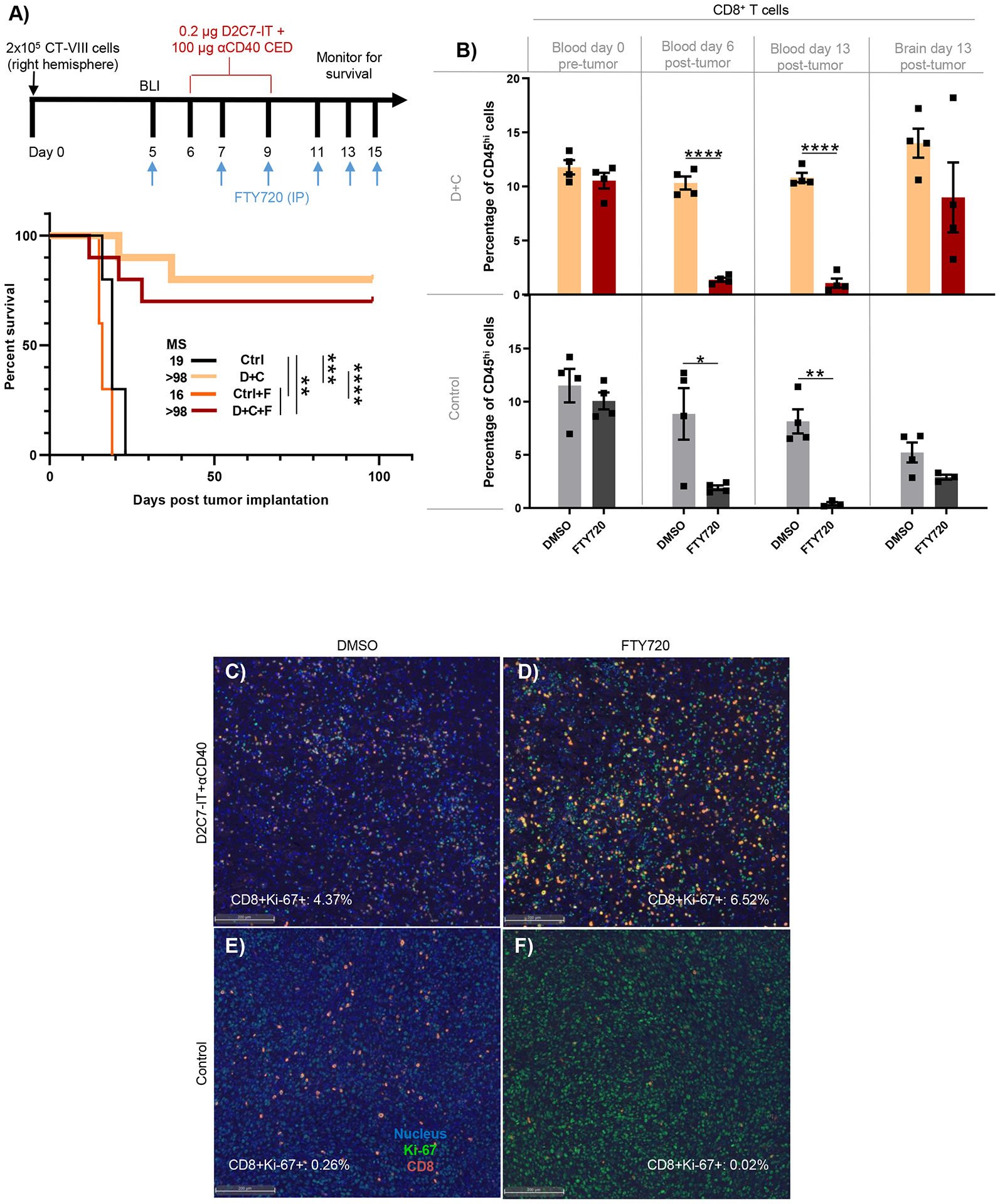
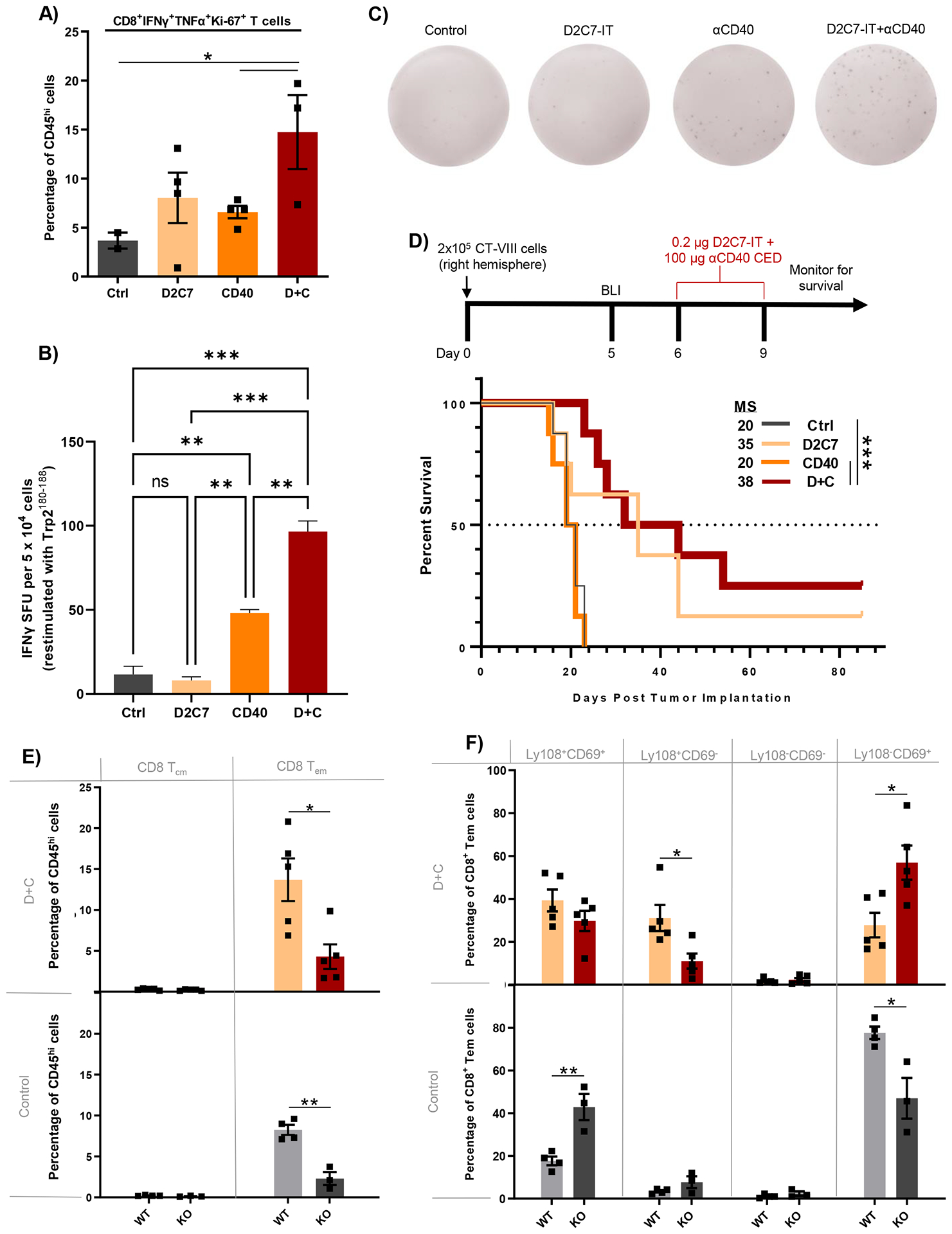
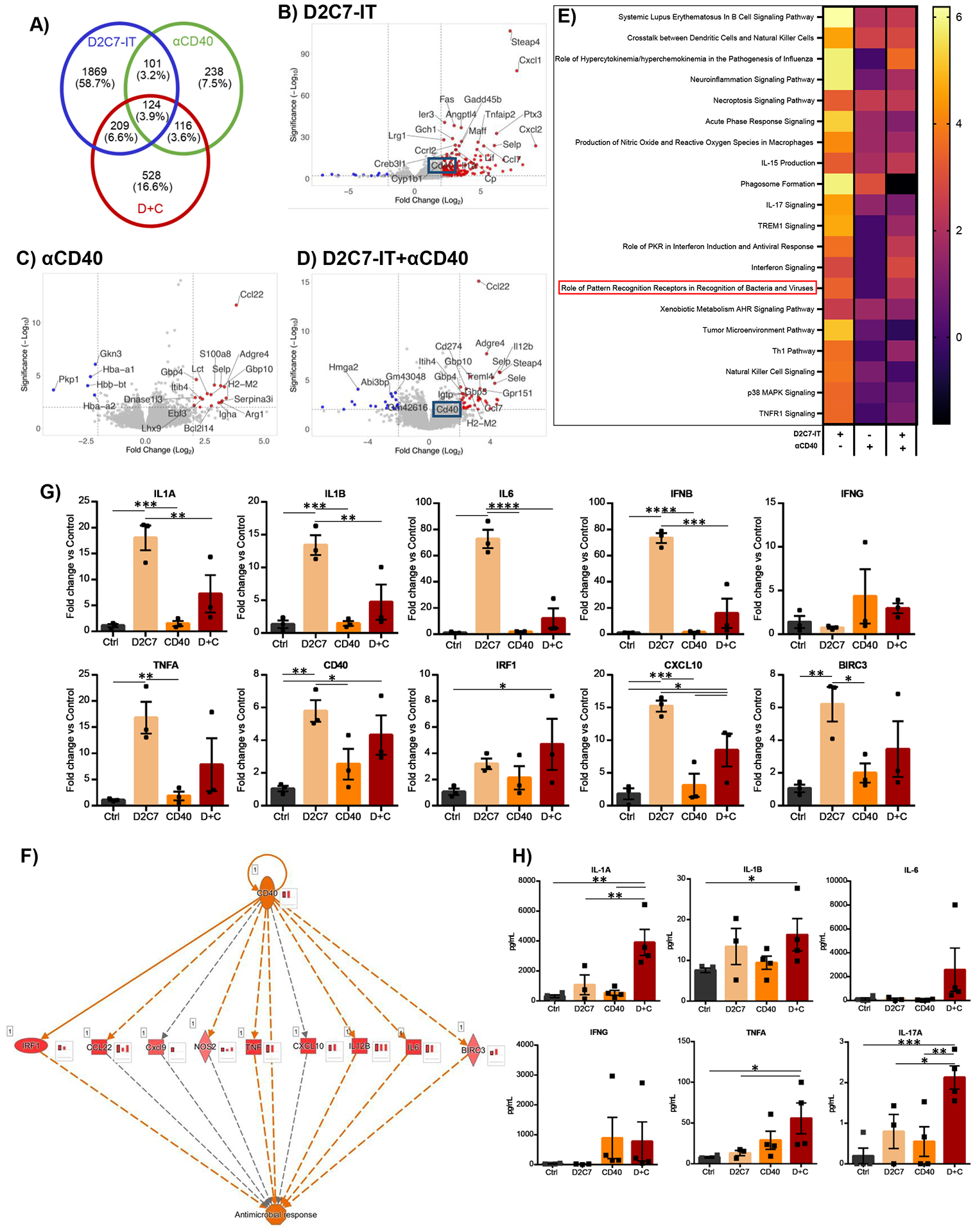
D2C7-immunotoxin (IT), a dual-specific IT targeting wild-type epidermal growth factor receptor (EGFR) and mutant EGFR variant III (EGFRvIII) proteins, demonstrates encouraging survival outcomes in a subset of patients with glioblastoma. We hypothesized that immunosuppression in glioblastoma limits D2C7-IT efficacy. To improve the response rate and reverse immunosuppression, we combined D2C7-IT tumor cell killing with αCD40 costimulation of antigen-presenting cells. In murine glioma models, a single intratumoral injection of D2C7-IT+αCD40 treatment activated a proinflammatory phenotype in microglia and macrophages, promoted long-term tumor-specific CD8+ T cell immunity, and generated cures. D2C7-IT+αCD40 treatment increased intratumoral Slamf6+CD8+ T cells with a progenitor phenotype and decreased terminally exhausted CD8+ T cells. D2C7-IT+αCD40 treatment stimulated intratumoral CD8+ T cell proliferation and generated cures in glioma-bearing mice despite FTY720-induced peripheral T cell sequestration. Tumor transcriptome profiling established CD40 up-regulation, pattern recognition receptor, cell senescence, and immune response pathway activation as the drivers of D2C7-IT+αCD40 antitumor responses. To determine potential translation, immunohistochemistry staining confirmed CD40 expression in human GBM tissue sections. These promising preclinical data allowed us to initiate a phase 1 study with D2C7-IT+αhCD40 in patients with malignant glioma (NCT04547777) to further evaluate this treatment in humans.
Conflict of interest statement
P.D. is an employee of Cytek Biosciences, Inc. V.C., D.D.B., and I.H.P. are inventors on patent application (DU6879US; Immunotherapy with combination therapy comprising an Immunotoxin) licensed to Vimana. D.D.B. serves as a consultant for Istari Oncology and Vimana. L.S.P. is currently an employee of Tune Therapeutics, Inc. A.B. is presently an employee of Xilis. A.M.S. is currently an employee of Immorna. T.F.T. is the founder of Cellective Biotherapy, Inc. and Antigenomycs, Inc., not related to the present work. A.D. serves as an advisory board member for Orbus Therapeutics and Midatech Pharma, served on the advisory board of Istari Oncology within the last two years, receives clinical research support (to the institution) from Orbus Therapeutics and Midatech Pharma, and has stock options with Istari Oncology. D.M.A. serves as an advisory board member for Immunogenesis, MAIA Biotechnology, and Diverse Biotech and a consultant for Jackson Laboratories. M.D.G. serves as an advisory board member for Myeloid Therapeutics. D.A.K. serves as an expert consultant for Shoreline Biosciences, not related to the present work. S.K.N. is a member of the Pfizer mRNA advisory panel, an inventor on patents licensed to Istari Oncology and Vimana, and a co-founder of NanoVenari Technologies, LLC. The other authors declare that they have no competing interests.
Figures

References
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO, European Organisation for R, Treatment T of Cancer Brain, G. Radiotherapy, G. National Cancer Institute of Canada Clinical Trials, Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352, 987–996 (2005). - PubMed
-
- Fernandes C, Costa A, Osorio L, Lago RC, Linhares P, Carvalho B, Caeiro C, in Glioblastoma, De Vleeschouwer S, Ed. (Codon Publications, 2017). - PubMed
-
- Cloughesy TF, Mochizuki AY, Orpilla JR, Hugo W, Lee AH, Davidson TB, Wang AC, Ellingson BM, Rytlewski JA, Sanders CM, Kawaguchi ES, Du L, Li G, Yong WH, Gaffey SC, Cohen AL, Mellinghoff IK, Lee EQ, Reardon DA, O’Brien BJ, Butowski NA, Nghiemphu PL, Clarke JL, Arrillaga-Romany IC, Colman H, Kaley TJ, de Groot JF, Liau LM, Wen PY, Prins RM, Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat Med 25, 477–486 (2019). - PMC - PubMed
-
- Desjardins A, Gromeier M, Herndon JE 2nd, Beaubier N, Bolognesi DP, Friedman AH, Friedman HS, McSherry F, Muscat AM, Nair S, Peters KB, Randazzo D, Sampson JH, Vlahovic G, Harrison WT, McLendon RE, Ashley D, Bigner DD, Recurrent Glioblastoma Treated with Recombinant Poliovirus. N Engl J Med 379, 150–161 (2018). - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
