

The role of hepatokines in NAFLD
- PMID: 36754018
- PMCID: PMC10157895
- DOI: 10.1016/j.cmet.2023.01.006
The role of hepatokines in NAFLD
Abstract
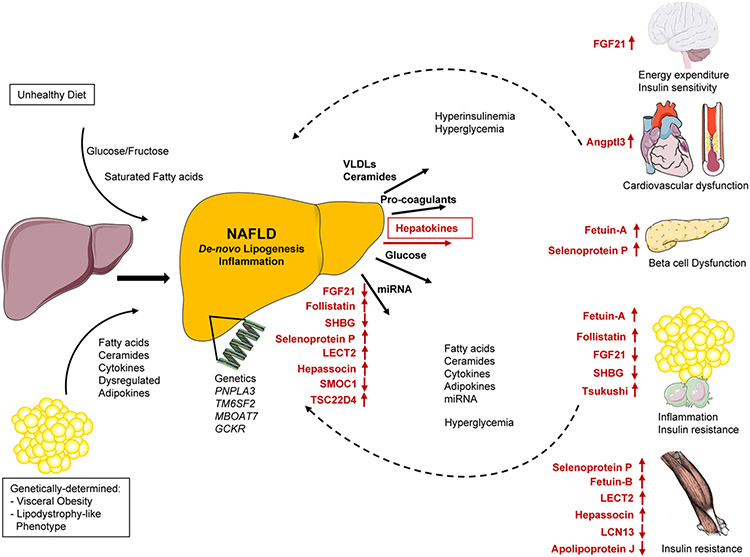
Non-alcoholic fatty liver disease (NAFLD) is not only a consequence of insulin resistance, but it is also an important cause of insulin resistance and major non-communicable diseases (NCDs). The close relationship of NAFLD with visceral obesity obscures the role of fatty liver from visceral adiposity as the main pathomechanism of insulin resistance and NCDs. To overcome this limitation, in analogy to the concept of adipokines, in 2008 we introduced the term hepatokines to describe the role of fetuin-A in metabolism. Since then, several other hepatokines were tested for their effects on metabolism. Here we address the dysregulation of hepatokines in people with NAFLD. Then, we discuss pathophysiological mechanisms of cardiometabolic diseases specifically related to NAFLD by focusing on hepatokine-related organ crosstalk. Finally, we propose how the determination of major hepatokines and adipokines can be used for pathomechanism-based clustering of insulin resistance in NAFLD and visceral obesity to better implement precision medicine in clinical practice.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests M.F.W. is an advisory board member of Housey Pharma (https://www.housey.com/).
Figures



References
-
- Mantovani A, Csermely A, Petracca G, Beatrice G, Corey KE, Simon TG, Byrne CD, and Targher G (2021). Non-alcoholic fatty liver disease and risk off atal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet. Gastroenterol. Hepatol 6, 903–913. 10.1016/S2468-1253(21)00308-3. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
