

Applicability of Vericiguat to Patients Hospitalized for Heart Failure in the United States
- PMID: 36754528
- PMCID: PMC11045268
- DOI: 10.1016/j.jchf.2022.11.007
Applicability of Vericiguat to Patients Hospitalized for Heart Failure in the United States
Abstract
Background: In January 2021, vericiguat, a soluble guanylate cyclase stimulator, was approved by the U.S. Food and Drug Administration (FDA) to reduce the risk of cardiovascular death and heart failure (HF) hospitalization among patients with a recent worsening HF event based on the VICTORIA (VerICiguaT Global Study in Subjects with Heart Failure with Reduced Ejection Fraction) trial.
Objectives: This study sought to leverage a contemporary U.S. registry of patients hospitalized for heart failure (HF) to characterize patients who may be candidates for vericiguat based on FDA label and the VICTORIA trial eligibility criteria.
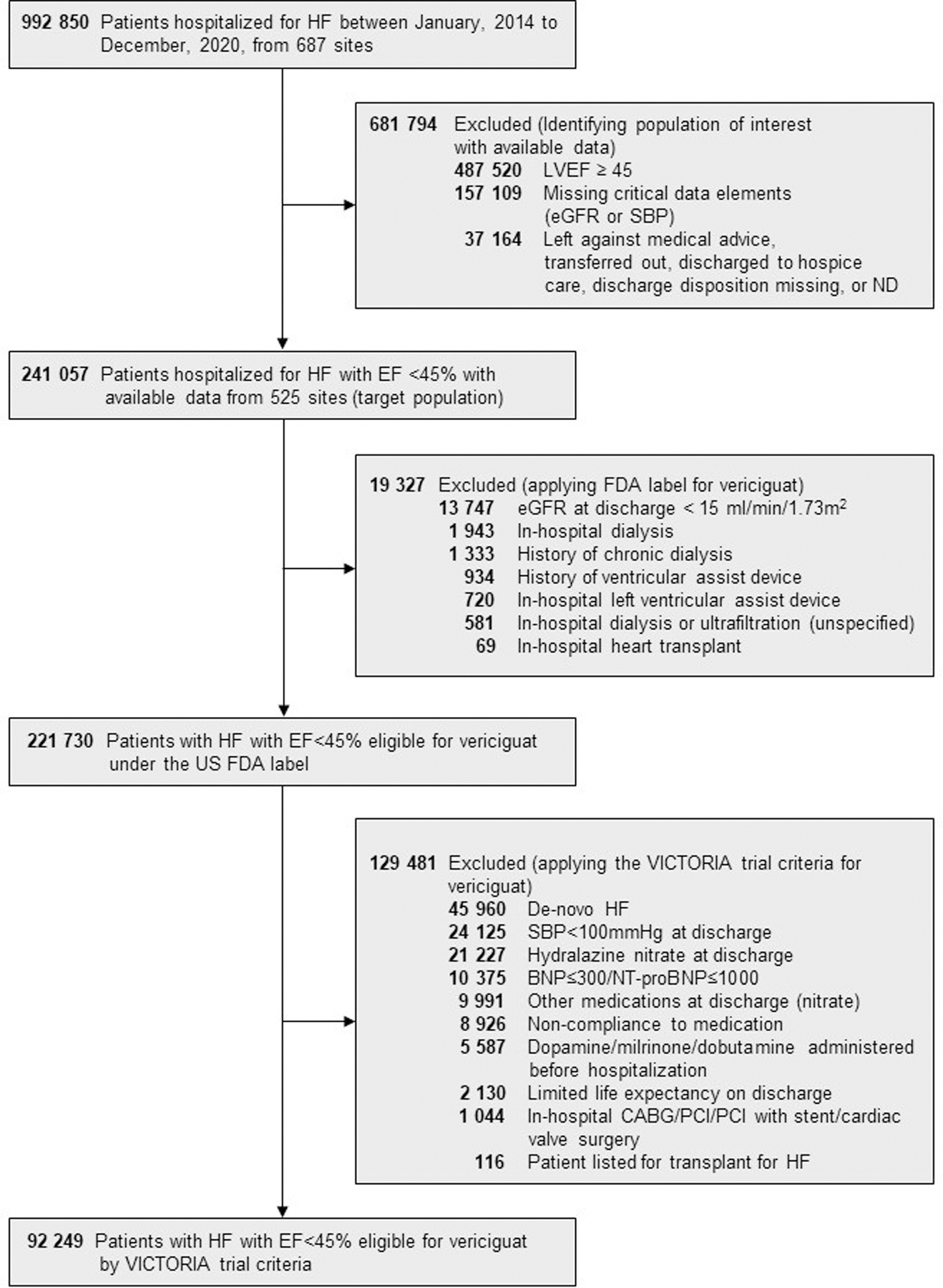
Methods: The authors studied patients hospitalized for HF with ejection fraction (EF) <45% across 525 sites in the GWTG-HF (Get With The Guidelines-Heart Failure) registry between January 2014 and December 2020. Approximate FDA label criteria (excluding estimated glomerular filtration rate [eGFR] <15 mL/min/1.73 m2, dialysis, or patients with heart transplantation or durable mechanical circulatory support) and eligibility criteria for the VICTORIA trial were applied to the GWTG-HF cohort.
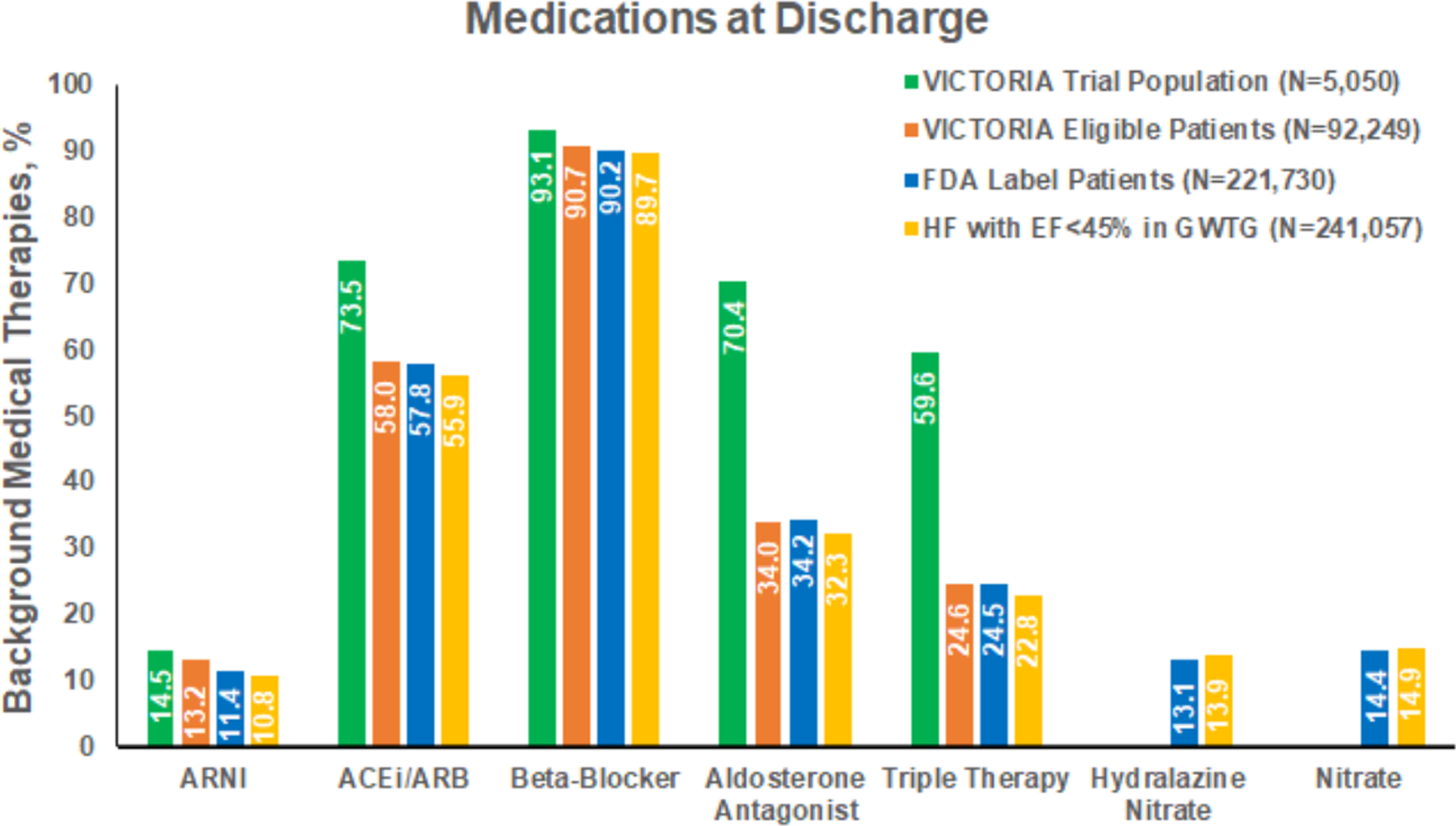
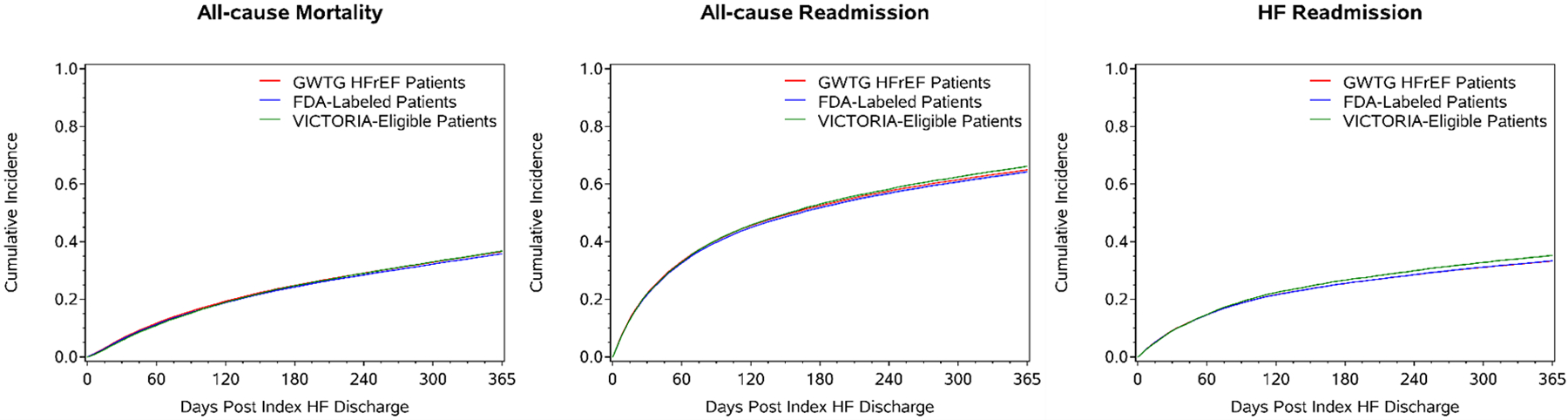
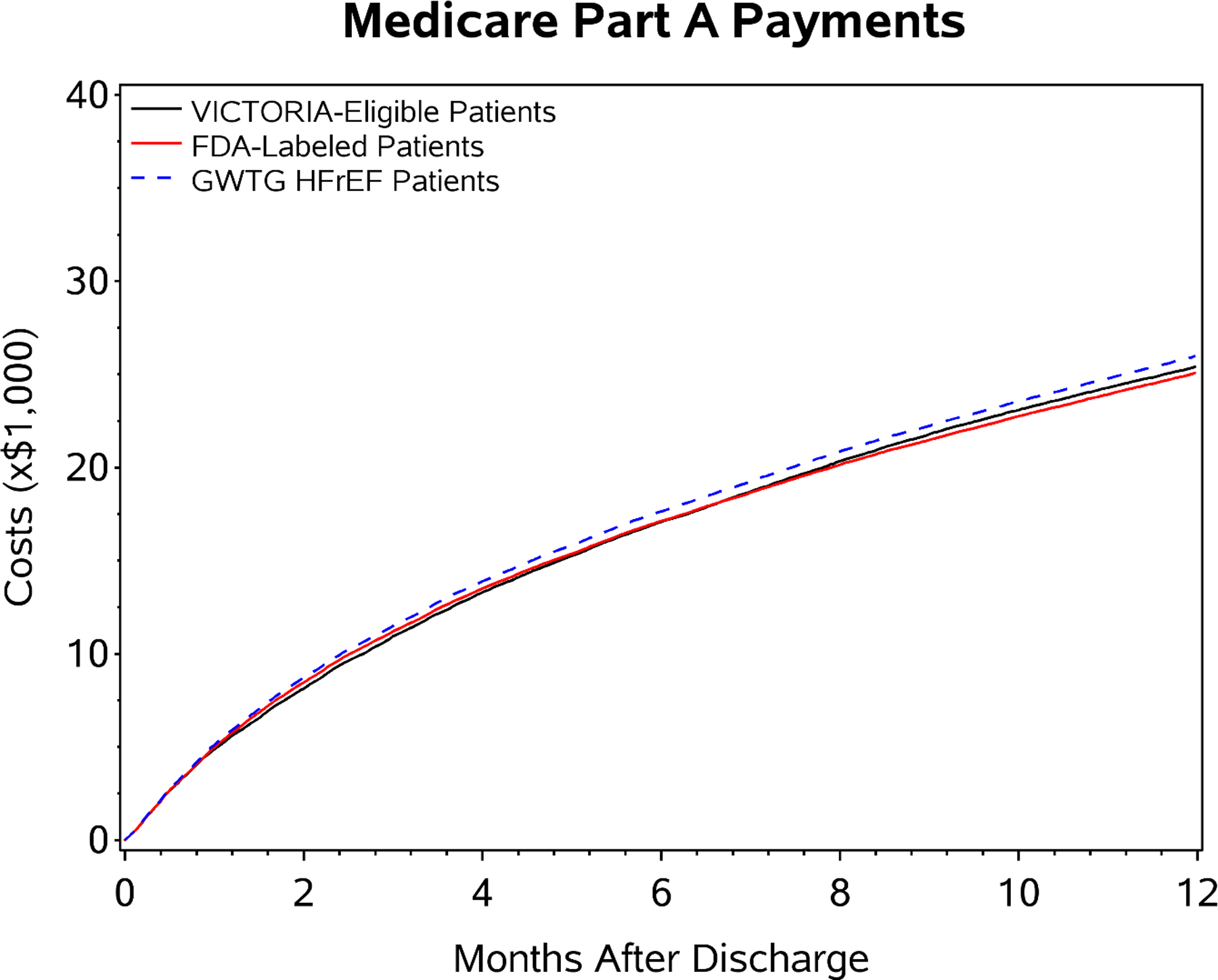
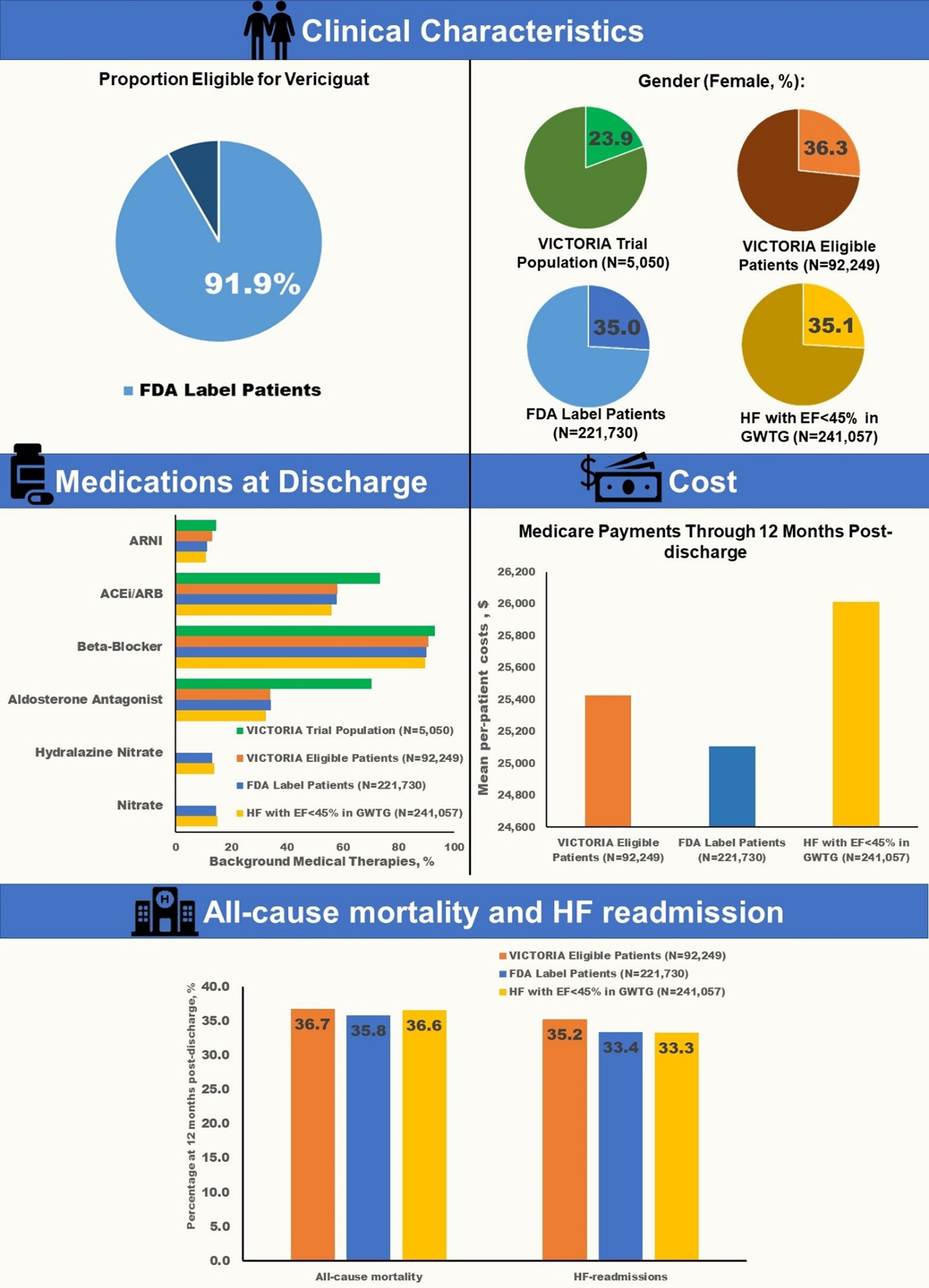
Results: Among 241,057 patients with EF <45% in the GWTG-HF registry, 221,730 (92%) could be candidates for vericiguat under the FDA label and 92,249 (38%) would have been eligible for the VICTORIA trial. The most frequent reasons for ineligibility for the FDA label were eGFR <15 mL/min/1.73 m2 (5.7%) and dialysis (1.6%). Although there were greater proportions of women and Black patients in the GWTG-HF registry, most clinical characteristics were qualitatively similar with patients enrolled in the VICTORIA trial. Among Medicare beneficiaries in the GWTG-HF registry eligible for vericiguat by either FDA label or VICTORIA trial criteria, 12-month postdischarge rates of mortality (36%-37%), HF hospitalization (33%-35%), all-cause hospitalization (64%-66%), and mean health care expenditure (U.S. $25,106-$25,428) were high.
Conclusions: Data from a large, contemporary U.S. registry of patients actively hospitalized for HF with EF <45% suggest that approximately 4 in 10 patients meet the criteria of the VICTORIA trial and that more than 9 in 10 patients are potential candidates for vericiguat based on the FDA label. Contemporary Medicare beneficiaries hospitalized for HF with EF <45% and eligible for vericiguat face high rates of postdischarge mortality and readmission and accrue substantial health care costs.
Keywords: heart failure; hospitalization; trial; vericiguat.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co, Inc (Rahway, New Jersey, USA). The Get With The Guidelines–Heart Failure program is provided by the American Heart Association and sponsored, in part, by Novartis, Boehringer Ingelheim and Eli Lilly Diabetes Alliance, Novo Nordisk, Sanofi, AstraZeneca, and Bayer. Dr Fonarow has served as a consultant for Abbott, Amgen, AstraZeneca, Bayer, Cytokinetics, Janssen, Medtronic, Merck Sharp & Dohme LLC (a subsidiary of Merck & Co, Inc), and Novartis. Drs Lautsch and Hilkert are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co, Inc. Dr Allen has received grant support from the National Institutes of Health and Patient-Centered Outcomes Research Institute; and has received consulting fees from ACI Clinical, American Heart Association, Boston Scientific, Cytokinetics, Novartis, and UpToDate. Dr Albert has received grant support from Novartis and AstraZeneca; and consulting fees from Boston Scientific, Boehringer Ingelheim/Lilly, Cytokinetics, and Merck Sharp & Dohme LLC (a subsidiary of Merck & Co, Inc). Dr Butler has served as a consultant for Abbott, Adrenomed, Arena Pharma, Array, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Cardior, CVRx, Eli Lilly, G3 Pharma, Imbria, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck Sharp & Dohme LLC (a subsidiary of Merck & Co, Inc), Novartis, Novo Nordisk, Sequana Medical, V-Wave Limited, and Vifor. Dr Greene has received research support from the Duke University Department of Medicine Chair’s Research Award, American Heart Association (#929502), National Heart, Lung, and Blood Institute, Amgen, AstraZeneca, Bristol Myers Squibb, Cytokinetics, Merck Sharp & Dohme LLC (a subsidiary of Merck & Co, Inc), Novartis, Pfizer, and Sanofi; served on the advisory board for Amgen, AstraZeneca, Boehringer Ingelheim/Lilly, Bristol Myers Squibb, Cytokinetics, Roche Diagnostics, scPharmaceuticals, and Sanofi; and served as a consultant for Amgen, Bayer, Boehringer Ingelheim/Lilly, Bristol Myers Squibb, CSL Vifor, Corteria Therapeutics, Merck Sharp & Dohme LLC (a subsidiary of Merck & Co, Inc), PharmaIN, Roche Diagnostics, Sanofi, Tricog Health, and Urovant Pharmaceuticals; and has received speaker fees from Boehringer Ingelheim and Cytokinetics. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Vericiguat in HFrEF: Insights From the GWTG-HF Registry.JACC Heart Fail. 2023 Feb;11(2):224-226. doi: 10.1016/j.jchf.2022.11.019. JACC Heart Fail. 2023. PMID: 36754529 No abstract available.
References
-
- Butler J, Yang M, Manzi MA et al. Clinical Course of Patients With Worsening Heart Failure With Reduced Ejection Fraction. J Am Coll Cardiol 2019;73:935–944. - PubMed
-
- Okumura N, Jhund PS, Gong J et al. Importance of Clinical Worsening of Heart Failure Treated in the Outpatient Setting: Evidence From the Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure Trial (PARADIGM-HF). Circulation 2016;133:2254–62. - PubMed
-
- Armstrong PW, Pieske B, Anstrom KJ et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2020;382:1883–1893. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022;79:e263–e421. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
