

Efficacy and clinicogenomic correlates of response to immune checkpoint inhibitors alone or with chemotherapy in non-small cell lung cancer
- PMID: 36755027
- PMCID: PMC9908867
- DOI: 10.1038/s41467-023-36328-z
Efficacy and clinicogenomic correlates of response to immune checkpoint inhibitors alone or with chemotherapy in non-small cell lung cancer
Abstract
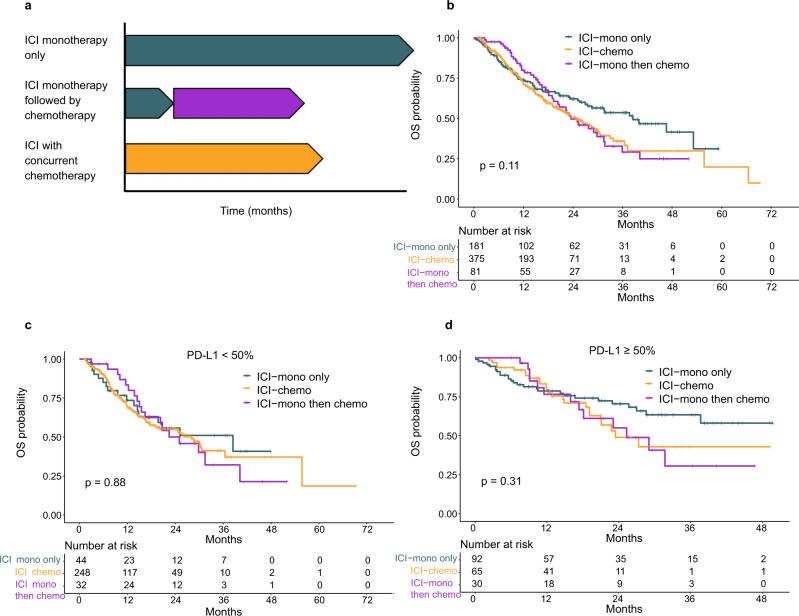
The role of combination chemotherapy with immune checkpoint inhibitors (ICI) (ICI-chemo) over ICI monotherapy (ICI-mono) in non-small cell lung cancer (NSCLC) remains underexplored. In this retrospective study of 1133 NSCLC patients, treatment with ICI-mono vs ICI-chemo associate with higher rates of early progression, but similar long-term progression-free and overall survival. Sequential vs concurrent ICI and chemotherapy have similar long-term survival, suggesting no synergism from combination therapy. Integrative modeling identified PD-L1, disease burden (Stage IVb; liver metastases), and STK11 and JAK2 alterations as features associate with a higher likelihood of early progression on ICI-mono. CDKN2A alterations associate with worse long-term outcomes in ICI-chemo patients. These results are validated in independent external (n = 89) and internal (n = 393) cohorts. This real-world study suggests that ICI-chemo may protect against early progression but does not influence overall survival, and nominates features that identify those patients at risk for early progression who may maximally benefit from ICI-chemo.
© 2023. The Author(s).
Conflict of interest statement
M.V.N. reports Research funding to institution from Mirati, Novartis, Alaunos, Checkmate, AstraZeneca, Pfizer, Genentech; and Consultant/Advisory Board from Mirati, Novartis, Genentech, and Merck/MSD, outside the submitted work. Y.Y.E. reports research support from Spectrum, AstraZeneca, Takeda, Eli Lilly, Xcovery, and Tuning Point Therapeutics; and advisory role for AstraZeneca, Eli Lilly, Sanofi, BMS, Spectrum and Turning Point; and accommodation expenses from Eli Lilly. F.S. reports consulting fees and advisory roles from Amgen Inc., AstraZeneca Pharmaceuticals, Novartis, BeiGene, Tango Therapeutics, Calithera Biosciences, Navire Pharma, Medscape LLC, Intellisphere LLC, Guardant Health, and BergenBio; speaker fees from BMS, RV MaisPromocao Eventos LTDS, the Visiting Speakers Program in Oncology at McGill University and the Universite´ de Montre´al, AIM Group International, and ESMO; fees for travel, food, and beverage from Tango Therapeutics, AstraZeneca Pharmaceuticals, Amgen Inc., Guardant Health, and Dava Oncology; stock or stock options in BioNTech SE and Moderna Inc.; research grants (to institution) from Amgen Inc., Mirati Therapeutics, Boehringer Ingelheim, Merck & Co, and Novartis; Study Chair funds (to institution) from Pfizer; and research grants (spouse, to institution) from Almmune. C.M.G. reports fees for advisory committees from AstraZeneca, Bristol Myers Squibb, Jazz Pharmaceuticals, G1 therapeutics, and Monte Rosa Therapeutics, research support from AstraZeneca, and speaker’s fees from AstraZeneca and Beigene. T.C. reports speaker fees/honoraria from the Society for Immunotherapy of Cancer (SITC), Bristol Myers Squibb, Roche, Medscape, IDEOlogy Health, Physicians’ Education Resource®, LLC (PER®), OncLive and PeerView; travel, food and beverage expenses from Physicians' Education Resource®, LLC (PER®), Dava Oncology, SITC, International Association for the Study of Lung Cancer, IDEOlogy Health and Bristol Myers Squibb; advisory role/consulting fees from MedImmune/AstraZeneca, Bristol Myers Squibb, EMD Serono, Merck, Genentech, Arrowhead Pharmaceuticals and Regeneron; and institutional research funding from MedImmune/AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim and EMD Serono, all outside of the submitted work. S.J.G. reports research support from AstraZeneca, BMS, and Millenium Pharmaceuticals, all outside of the submitted work. P.P.L. reports personal fees from Viewray, Inc., AstraZeneca, Inc., personal fees and non-financial support from Varian, Inc., personal fees from Genentech, Inc., outside the submitted work. D.L.G. reports honoraria for scientific advisory boards from AstraZeneca, Sanofi, Alethia Biotherapeutics, Menarini, Eli Lilly, 4D Pharma and Onconova, and research support from Janssen, Takeda, Astellas, Ribon Therapeutics, NGM Biopharmaceuticals, Boehringer Ingelheim, Mirati Therapeutics and AstraZeneca, all outside of the submitted work. X.L. reports receiving consultant and advisory fee from Eli Lilly, AstraZeneca, EMD Serono, Daiishi Sanko, Spectrum Therapeutics, Boehringer Ingelheim, Hengrui Therapeutics, Novartis, and research funding from Eli Lilly, Boehringer Ingelheim, all outside of the submitted work. J.F.G. has served as a compensated consultant or received honoraria from Bristol-Myers Squibb, Genentech/Roche, Takeda, Loxo/Lilly, Blueprint, AstraZeneca, Gilead, Moderna, AstraZeneca, Curie Therapeutics, Mirati, Nuvalent, Pfizer, Novartis, Merck, iTeos, Karyopharm, Silverback Therapeutics, and GlydeBio; research support from Novartis, Genentech/Roche, and Takeda; institutional research support from Bristol-Myers Squibb, Tesaro, Moderna, Blueprint, Jounce, Array Biopharma, Merck, Adaptimmune, Novartis, and Alexo; and has an immediate family member who is an employee with equity at Ironwood Pharmaceuticals. J.V.H. reports receiving advisory/consulting fees from AstraZeneca, Boehringer-Ingeheim, Catalyst, Genentech, GlaxoSmithKline, Guardant Health, Foundation Medicine, Hengrui Therapeutics, Eli Lilly, Novartis, Spectrum, Sanofi, Takeda Pharmaceuticals, Mirati Therapeutics, Bristiol-Myers Squibb, BrightPath Biotherapeutics, Janssen Global Services, Nexus Health Systems, EMD Serono, Pneuma Respiratory, Kairos Venture Investments, Leads Biolabs, RefleXion, and research funding from GlaxoSmithKline, AstraZeneca, Spectrum, all outside of the submitted work. Y.L. reports research funding from Merck, MacroGenics, Tolero Pharmaceuticals, AstraZeneca, Vaccinex, Blueprint Medicines, Harpoon Therapeutics, Sun Pharma Advanced Research, Bristol-Myers Squibb, Kyowa Pharmaceuticals, Tesaro, Bayer HealthCare, Mirati Therapeutics, Daiichi Sankyo. Scientific Advisory boards for AstraZeneca Pharmaceuticals, Janssen Pharmaceutical, Lilly Oncology, Turning point therapeutics. Consultation fee from AstraZeneca. Honorarium from Clarion Health Care. J.Z. reports grants from Merck, Novartis, Johnson and Johnson, personal fees from BMS, AZ, Novartis, Johnson and Johnson, GenePlus, Hengrui, Innovent, outside the submitted work. N.I.V. receives consulting fees from Sanofi, Regeneron, Oncocyte, and Eli Lilly, and research funding from Mirati, outside the submitted work. The other authors declare no competing interests in the submitted work.
Figures





References
-
- Herbst RS, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387:1540–1550. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
