

Rule-out of non-ST-segment elevation acute coronary syndrome by a single, pre-hospital troponin measurement: a randomized trial
- PMID: 36755110
- PMCID: PMC10182886
- DOI: 10.1093/eurheartj/ehad056
Rule-out of non-ST-segment elevation acute coronary syndrome by a single, pre-hospital troponin measurement: a randomized trial
Abstract
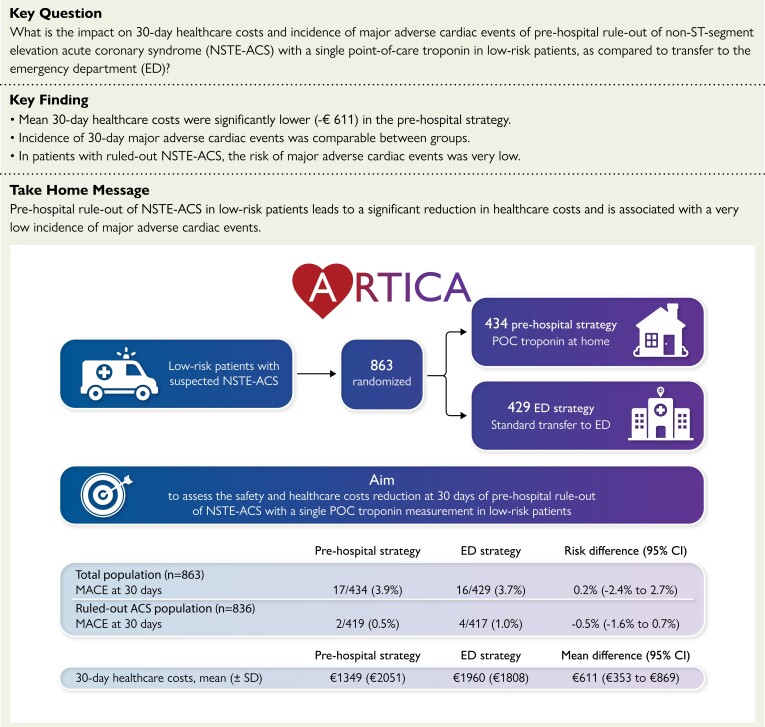
Aims: Patients with suspected non-ST-segment elevation acute coronary syndrome (NSTE-ACS) are routinely transferred to the emergency department (ED). A clinical risk score with point-of-care (POC) troponin measurement might enable ambulance paramedics to identify low-risk patients in whom ED evaluation is unnecessary. The aim was to assess safety and healthcare costs of a pre-hospital rule-out strategy using a POC troponin measurement in low-risk suspected NSTE-ACS patients.
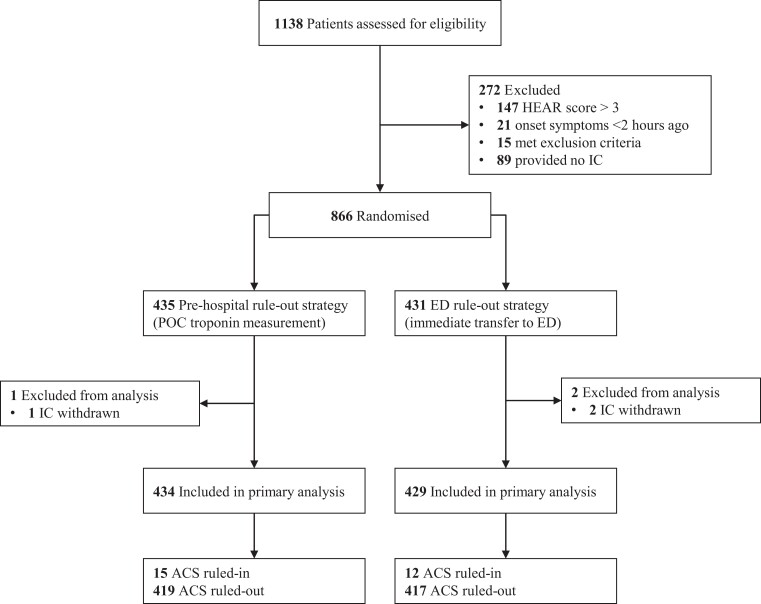
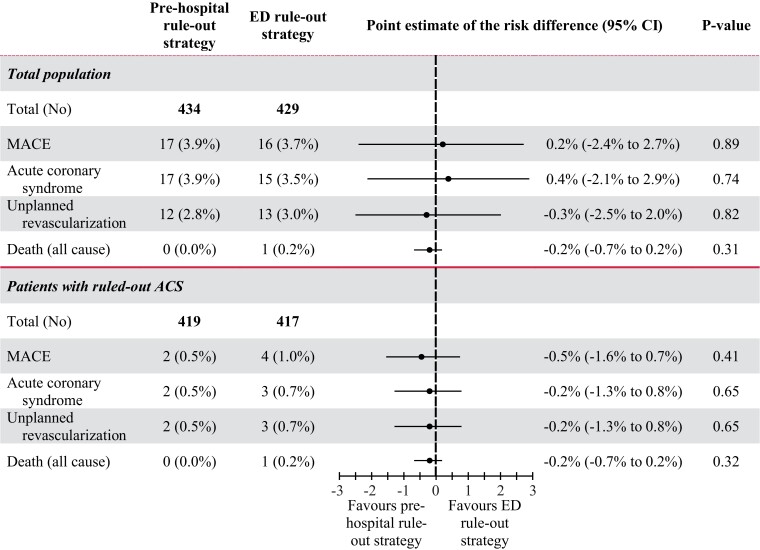
Methods and results: This investigator-initiated, randomized clinical trial was conducted in five ambulance regions in the Netherlands. Suspected NSTE-ACS patients with HEAR (History, ECG, Age, Risk factors) score ≤3 were randomized to pre-hospital rule-out with POC troponin measurement or direct transfer to the ED. The sample size calculation was based on the primary outcome of 30-day healthcare costs. Secondary outcome was safety, defined as 30-day major adverse cardiac events (MACE), consisting of ACS, unplanned revascularization or all-cause death. : A total of 863 participants were randomized. Healthcare costs were significantly lower in the pre-hospital strategy (€1349 ± €2051 vs. €1960 ± €1808) with a mean difference of €611 [95% confidence interval (CI): 353-869; P < 0.001]. In the total population, MACE were comparable between groups [3.9% (17/434) in pre-hospital strategy vs. 3.7% (16/429) in ED strategy; P = 0.89]. In the ruled-out ACS population, MACE were very low [0.5% (2/419) vs. 1.0% (4/417)], with a risk difference of -0.5% (95% CI -1.6%-0.7%; P = 0.41) in favour of the pre-hospital strategy.
Conclusion: Pre-hospital rule-out of ACS with a POC troponin measurement in low-risk patients significantly reduces healthcare costs while incidence of MACE was low in both strategies.
Trial registration: Clinicaltrials.gov identifier NCT05466591 and International Clinical Trials Registry Platform id NTR 7346.
Keywords: Acute coronary syndrome; HEART score; Point-of-care troponin; Pre-hospital triage; Risk stratification.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest C.C. reports a grant from ZonMw (The Netherlands Organisation for Health Research and Development) and consulting fees from AstraZeneca and Xenikos BV; R.R.J.v.K. reports honoraria grants from Bayer and Novartis, P.D. reports grants from Philips, Abbott and AstraZeneca and consulting fees from Philips; N.v.R. reports grants from Abbott, Philips, Medtronic and Biotronik and speaker fees from Microport, Abbott, Rainmed and Bayer. The other authors have no conflicts of interest.
Figures
Comment in
-
To be or not to be admitted to the emergency department for chest pain? A costly dilemma.Eur Heart J. 2023 May 14;44(19):1715-1717. doi: 10.1093/eurheartj/ehad116. Eur Heart J. 2023. PMID: 36918747 No abstract available.
References
-
- Writing Committee Members, Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, et al. . 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol 2021;78:e187–e285. 10.1016/j.jacc.2021.07.053 - DOI - PubMed
-
- Pitts SR, Niska RW, Xu J, Burt CW. National hospital ambulatory medical care survey: 2006 emergency department summary. Natl Health Stat Report 2008;7:1–38. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
