

Economic costs, health-related quality of life outcomes and cost-utility of a physical and psychological group intervention targeted at older adults with neurogenic claudication
- PMID: 36755265
- PMCID: PMC9906820
- DOI: 10.1186/s12962-022-00410-y
Economic costs, health-related quality of life outcomes and cost-utility of a physical and psychological group intervention targeted at older adults with neurogenic claudication
Erratum in
-
Correction to: Economic costs, health-related quality of life outcomes and cost-utility of a physical and psychological group intervention targeted at older adults with neurogenic claudication.Cost Eff Resour Alloc. 2023 Apr 11;21(1):24. doi: 10.1186/s12962-023-00431-1. Cost Eff Resour Alloc. 2023. PMID: 37041559 Free PMC article. No abstract available.
Abstract
Background: Emerging evidence suggests that structured and progressive exercise underpinned by a cognitive behavioural approach can improve functional outcomes in patients with neurogenic claudication (NC). However, evidence surrounding its economic benefits is lacking.
Objectives: To estimate the economic costs, health-related quality of life outcomes and cost-effectiveness of a physical and psychological group intervention (BOOST programme) versus best practice advice (BPA) in older adults with NC.
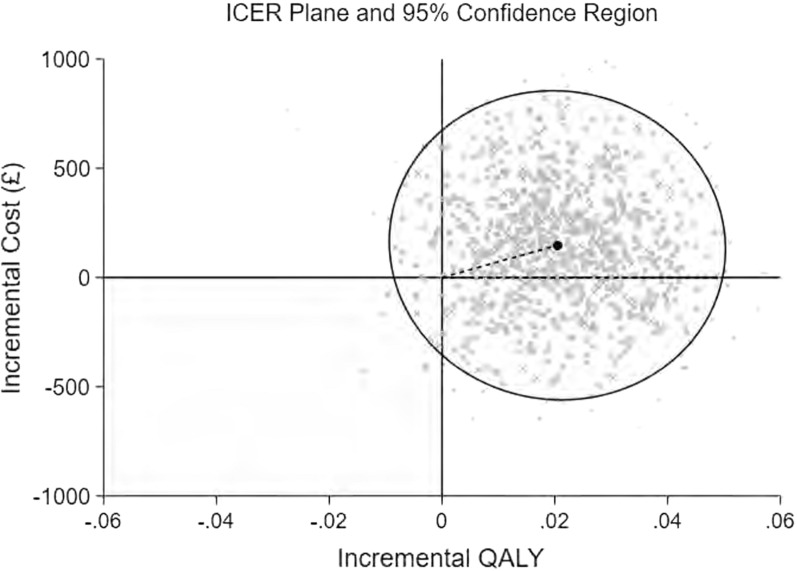
Methods: An economic evaluation was conducted based on data from a pragmatic, multicentre, superiority, randomised controlled trial. The base-case economic evaluation took the form of an intention-to-treat analysis conducted from a UK National Health Service (NHS) and personal social services (PSS) perspective and separately from a societal perspective. Costs (£ 2018-2019 prices) were collected prospectively over a 12 month follow-up period. A bivariate regression of costs and quality-adjusted life-years (QALYs), with multiple imputation of missing data, was conducted to estimate the incremental cost per QALY gained and the incremental net monetary benefit (INMB) of the BOOST programme in comparison to BPA. Sensitivity and pre-specified subgroup analyses explored uncertainty and heterogeneity in cost-effectiveness estimates.
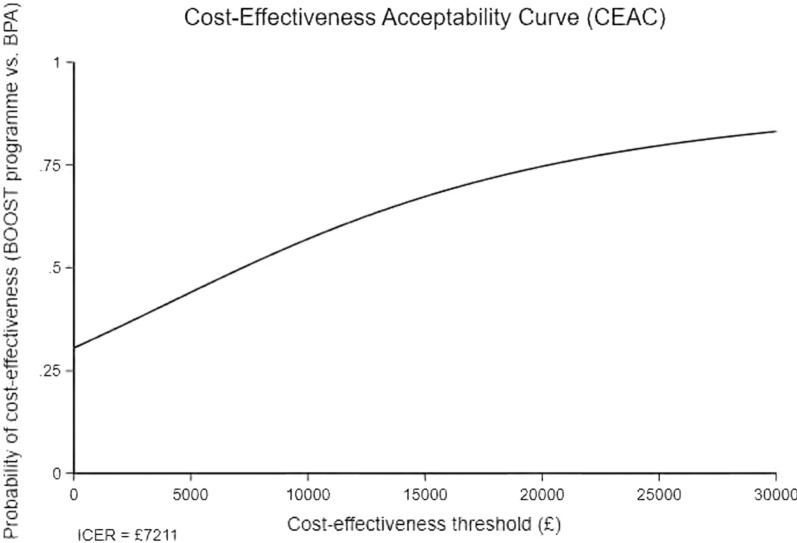
Results: Participants (N = 435) were randomised to the BOOST programme (n = 292) or BPA (n = 143). Mean (standard error [SE]) NHS and PSS costs over 12 months were £1,974 (£118) in the BOOST arm versus £1,827 (£169) in the BPA arm (p = 0.474). Mean (SE) QALY estimates were 0.620 (0.009) versus 0.599 (0.006), respectively (p = 0.093). The probability that the BOOST programme is cost-effective ranged between 67 and 83% (NHS and PSS perspective) and 79-89% (societal perspective) at cost-effectiveness thresholds between £15,000 and £30,000 per QALY gained. INMBs ranged between £145 and £464 at similar cost-effectiveness thresholds. The cost-effectiveness results remained robust to sensitivity analyses.
Conclusions: The BOOST programme resulted in modest QALY gains over the 12 month follow-up period. Future studies with longer intervention and follow-up periods are needed to address uncertainty around the health-related quality of life impacts and cost-effectiveness of such programmes. Trial registration This study has been registered in the International Standard Randomised Controlled Trial Number registry, reference number ISRCTN12698674. Registered on 10 November 2015.
Keywords: Cost-effectiveness; Economic costs; Exercise; Health-related quality of life; Neurogenic claudication; Psychosocial; Rehabilitation; Spinal stenosis.
© 2023. The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Does Structured Exercise Improve Cognitive Impairment in People with Mild to Moderate Dementia? A Cost-Effectiveness Analysis from a Confirmatory Randomised Controlled Trial: The Dementia and Physical Activity (DAPA) Trial.Pharmacoecon Open. 2019 Jun;3(2):215-227. doi: 10.1007/s41669-018-0097-9. Pharmacoecon Open. 2019. PMID: 30206826 Free PMC article.
-
Improving the understanding and management of back pain in older adults: the BOOST research programme including RCT and OPAL cohort.Southampton (UK): National Institute for Health and Care Research; 2023 Nov. Southampton (UK): National Institute for Health and Care Research; 2023 Nov. PMID: 38127693 Free Books & Documents. Review.
-
Subthreshold micropulse laser versus standard laser for the treatment of central-involving diabetic macular oedema with central retinal thickness of <400µ: a cost-effectiveness analysis from the DIAMONDS trial.BMJ Open. 2023 Oct 18;13(10):e067684. doi: 10.1136/bmjopen-2022-067684. BMJ Open. 2023. PMID: 37852765 Free PMC article. Clinical Trial.
-
Better Outcomes for Older people with Spinal Trouble (BOOST) Trial: a randomised controlled trial of a combined physical and psychological intervention for older adults with neurogenic claudication, a protocol.BMJ Open. 2018 Oct 18;8(10):e022205. doi: 10.1136/bmjopen-2018-022205. BMJ Open. 2018. PMID: 30341124 Free PMC article.
-
A cost-utility analysis comparing endovascular coiling to neurosurgical clipping in the treatment of aneurysmal subarachnoid haemorrhage.Neurosurg Rev. 2022 Oct;45(5):3259-3269. doi: 10.1007/s10143-022-01854-9. Epub 2022 Sep 3. Neurosurg Rev. 2022. PMID: 36056977 Free PMC article.
References
-
- Ammendolia C, Côté P, Southerst D, Schneider M, Budgell B, Bombardier C, Hawker G, Rampersaud YR. Comprehensive nonsurgical treatment versus self-directed care to improve walking ability in lumbar spinal stenosis: a randomized trial. Arch Phys Med Rehabil. 2018;99:2408–2419.e2402. doi: 10.1016/j.apmr.2018.05.014. - DOI - PubMed
-
- Minetama M, Kawakami M, Teraguchi M, Kagotani R, Mera Y, Sumiya T, Nakagawa M, Yamamoto Y, Matsuo S, Sakon N, et al. Supervised physical therapy versus unsupervised exercise for patients with lumbar spinal stenosis: 1-year follow-up of a randomized controlled trial. Clin Rehabil. 2021;35:964–975. doi: 10.1177/0269215520986688. - DOI - PubMed
-
- Khan I, Petrou S, Khan K, Mistry D, Lall R, Sheehan B, Lamb S. Does structured exercise improve cognitive impairment in people with mild to moderate dementia? a cost-effectiveness analysis from a confirmatory randomised controlled trial: the dementia and physical activity (DAPA) trial. Pharmaco Economics Open. 2019;3:215–227. doi: 10.1007/s41669-018-0097-9. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
